
Always keen to provoke doctors, Professor Chris Ham, head of the wealthiest and most influential health think-tank in the UK, The Kings Fund asked yesterday,
He received a predictable mixture of replies, but the most important was from Public Health consultant Gabriel Scally,
https://twitter.com/GabrielScally/status/582466901038764033
https://twitter.com/GabrielScally/status/582470626033709057
Last week a group of Hackney GPs working for our locally run, managed and operated, not-for-profit out of hours provider CHUHSE met to discuss our clinical audit tool called Clinical Guardian. We were joined by a director from another Out of Hours provider who described how it was developed and how useful it has been.
Clinical Guardian allows all the documented cases to be looked at anonymously by other clinicians so that the quality can be assessed. They look at 25% of each clinician’s cases and give each case a rating of ‘excellent’, ‘good’, ‘satisfactory’, ‘reflection’ or ‘concern’. These are then compared with the average results for other clinicians to give a performance summary. The one below is mine and you can see that I come out below average.
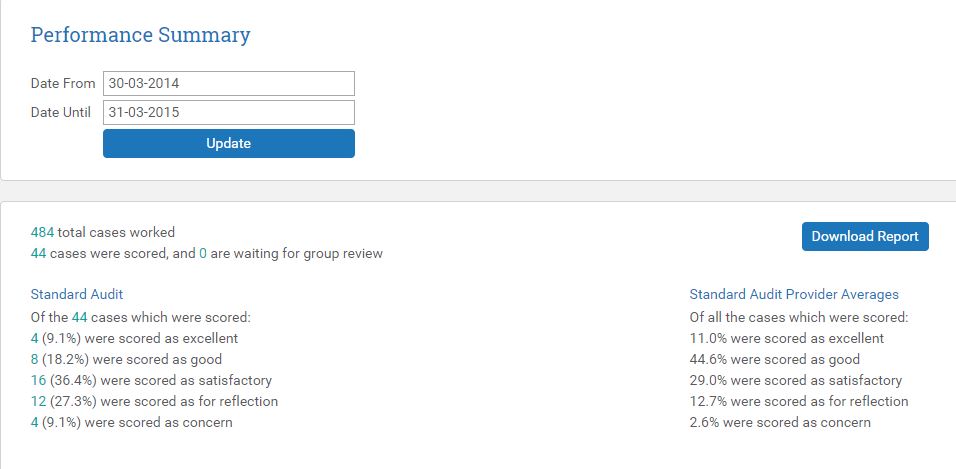
This puts me in an amber category so that next month they will look at 25% of my cases again. If I improve (I know what I have to do and sincerely hope I do!) I might improve enough to move up to a blue or green category and only 10% of my cases will be reviewed. Cases that are graded for ‘concern’ are immediately emailed to the clinician concerned and cases for reflection can be responded to on the Clinical Guardian website. One of my cases for concern was a woman who might have had a DVT. I thought she could wait until the morning before assessment but the team disagreed. Cases for reflection in my case were usually because I had failed to document enough detail.
The experience of the doctors working in Bristol was that continually auditing their doctors’ work and discussing cases significantly improved the quality of their documentation and the safety of patient care.
When I was flagged up as ‘amber’ I was asked to meet with two of our other out of hours GPs and we discussed all the cases for concern over the course of an hour in a critical, but friendly, educational supervisory session. I’m very used to clinical supervision and opening my practice up to scrutiny which undoubtedly softened the blow, but many GPs and consultants spend their lives working without ever having their practice inspected and audited like this.
The meeting last week with other GPs was, at times tense. They didn’t like being being judged on documentation that stripped a consultation of all the vital elements and quality markers of rapport, empathy, compassion, hands-on-skill, complex-shared-decision making and confidence-building. Nor does it include what patients thought of the consultation, although feedback for CHUHSE has been excellent. This audit looks only at the quality of documentation which is only one element of quality care, but nevertheless, we all agreed, an important one. In time, as we discussed our concerns, we gradually came around to the conclusion that a process of regular clinical audit and personal feedback – especially with an emphasis on education and support would be good for us, our patients and CHUHSE.
I’ve looked at the evidence and argued in a forthcoming paper that every clinician should have regular clinical supervision for as long as they are involved in patient care. The clinical uncertainty, ethical complexity and emotional engagement that we face does not fade with experience. I recently had the opportunity to go to a Schawartz round in a London hospital where a panel that included a consultant and a junior nurse sat in front of an audience that included any member of the trust who chose to come – there were all types of doctors, nurses, physiotherapists, and more. The panel presented a case that for them was especially important. The consultant began, but before he could finish was choked with tears. A facilitator sensitively introduced the next speaker while he composed himself and he later finished his version of the events. The details of the case, I’ll not share out of respect for confidentiality. The round lasted for an hour and the audience were invited to respond. In some ways it resembled a large Balint group, except that comments could be directed to the panel and they could respond. The facilitators explained that we weren’t there to give advice, so much as help them make sense of what had happened. We were especially moved by the nurse who said at the end, “I thought it was only the most junior members of staff who felt like this”. It is through role-modelling that virtues such as humility are learned and younger clinicians learn that vulnerability is normal.
When I (or indeed, almost any clinician) discusses the intensity of clinical practice, other professionals such as social workers or psychologists for whom clinical supervision is an essential part of their work, are astonished that we go without.
If we are to survive and sustain high-quality, safe and compassionate care in the face of unprecedented demands to do ever more with ever less, we need to support one-another. One of the best ways to do this is to open our practice and ourselves up to clinical audit and regular supervision- within a supportive, ‘just-culture’. As Don Berwick said after Mid Staffs,
The most powerful foundation for advancing patient safety in the NHS lies much more in its potential to be a learning organisation, than in the top down mechanistic imposition of rules, incentives and regulations.
Further reading:
“We view clinical supervision not as something imposed on medical professionals by their regulators, managers or those responsible for their ongoing training but rather something to be provided for and championed by doctors as something that helps them in their professional lives. In a world where pressures on many professions seem to increase almost logarithmically, it becomes harder to create the space for reflection – and yet that is when it is most needed”. Highly recommended Book: Clinical Supervision in the Medical Profession
Moving on from Balint: Embracing Clinical Supervision. Essay by John Launer
