
(Notes for my lecture to the North and East London GP Educators’ conference)
Introduction
At my last appraisal, I was criticised for not having more clinical conditions in my CPD (Continuing Professional Development) – “where” my appraiser asked, “was kidney disease, asthma, Diabetes, and Heart Failure?” I couldn’t think of an answer, it wasn’t that I was short of CPD, it’s just that my learning needs, the things I struggled with most as a GP were my difficulties in trying to help people with chronic pain, anxiety and depression, loneliness, severe obesity, shame, self-loathing and self-harm – the consequences of deprivation and adverse childhood experiences. It wasn’t that they weren’t also suffering from heart and lung disease and the rest – they were, to a huge extent, it’s just that managing these diseases wasn’t half as challenging as the rest. And most of the time it didn’t seem to be the cause of my patients’ greatest suffering.
GPs and lonely patients: Blogpost
How doctors respond to chronic pain: Blogpost
Doctors, patients and obesity: Blogpost
Anxiety and the medical profession: Blogpost
It was several months later that I watched a presentation by Professor Graham Watt from Glasgow University General Practice at the Deep End in which he explained that GPs working in practices serving the most disadvantaged patients have our own CPD needs. It was at this point that I realised that there is no curriculum for General Practice in deprived areas. As a GP registrar, I went on a ‘mountain medicine’ course, but I have never been on, or even seen a course called, ‘poverty medicine’. There are conferences dedicated to medicine for the homeless, and others centred around specific needs, such as addiction, but in poverty medicine addiction comes with depression, Hepatitis C, lung-cancer and COPD and frequent disruptions in care due to prison sentences.
David Hilfiker [an American GP from urban Minnesota, quoted in Arthur Frank’s wonderful book, The Renewal of Generosity] believes that the medical profession has lost its own moral ground with its deprecation of his work, which he calls “poverty medicine” …
There is no [medical school] curriculum for poverty medicine: no one teaches “The Art of Medical Decision Making With Limited Funds” or “Medical Compromise with Cultural Strictures”. Medical practice in a community of poor people often seems a solitary specialty without research, common cause, or shared-experience.
For Hilfiker, demoralisation in poverty medicine is the daily need for “almost indecent compromise of professional standards.”
George Bernard Shaw, in his preface to The Doctor’s dilemma wrote, over 100 years ago,
“When you [as a doctor] are so poor that you cannot afford to refuse eighteenpence from a man who is too poor to pay you any more, it is useless to tell him that what he or his sick child needs is not medicine, but more leisure, better clothes, better food and a better drained and ventilated house. It is kinder to give him a bottle of something almost as cheap as water and tell him to come again with another eighteenpence if it does not cure him.”
And which of us here today has not prescribed Sertraline or Pregabalin in similar circumstances?
“When you have done that over-and-over again every day for a week, how much scientific conscience have you left? A doctor’s character can no more stand out against such conditions as the lungs of his patients can stand out against bad ventilation. The only way in which he can preserve his self-respect is by forgetting all he ever learnt of science, and clinging to such help as he can give without cost merely by being less ignorant and more accustomed to sickbeds than his patients.” “Finally,” says Shaw, “The doctor acquires the skills of caring for patients under poverty-stricken conditions”
The curriculum that is notable by its absence is not hidden, but ‘null’ or ‘silent’. Is it only acquired with experience or could we, as trainers and educators help devise one? What would be on such a curriculum and how should it be taught?
GPs from the Deep End project in Glasgow identified the following as their top three CPD needs
- How to promote and maintain therapeutic optimism when working in areas of high deprivation
- How to address low patient engagement in health care and increase health literacy
- How to use EBM effectively when working with patients with high levels of multimorbidity and social complexity
One criticism GPs at the Deep End have had about the project is that it has had little impact on their day to day practice. This is something I would like to address today, by focussing on how the relationships between doctors and patients are affected in Poverty Medicine and what we can do to strengthen them.

Lesson 1:
Poverty medicine is emotional labour.
Sandra is severely obese and suffers from Type 2 diabetes, Asthma, COPD, eczema, diverticulitis, chronic back pain, chronic depression and severe, generalised anxiety and panic attacks. She rarely leaves her house, frequently fails to attend routine reviews and calls the surgery or out of hours service in times of crisis. She is prescribed insulin and another 10 daily medications, not including topical treatments. When she does come in she presents with pain (which I cannot diagnose), insomnia (which I cannot treat) or distress due to problems like abusive neighbours or a forthcoming benefits assessment (over which I feel I have little influence). It’s almost impossible to get on top of her dreadfully high blood sugars, her desperately under-treated COPD or her persistent psychology appointment DNAs.
Poverty medicine is emotional labour. We should be under no illusions about this. Patients like Sandra might be described in less deprived areas as occasional ‘heartsinks’ but where I work, patients like Sandra are our stock in trade. When my new registrar started at the beginning of February, she watched a surgery with me where 15/20 patients had a history of childhood sexual abuse, domestic violence or torture. Research from the General Practice at the Deep End project – a network of 100 of the most deprived GP practices in Glasgow showed GPs were having to manage more complex multimorbidity, with over twice the rate of mental health and social problems, in a greater proportion of their patients, who attended more frequently, at a younger age than patients in less deprived practices, with no more time, money or human resources, without specialist training or support.
We need to be honest with ourselves and our trainees about the personal impact of working with patients like this under these conditions. I recently ran a session for about 30 Hackney VTS trainees and one thing they wanted me to pass on was for us to be honest about how stressed and anxious our work makes us feel. The majority of them said they wouldn’t tell their trainer how anxious or stressed they felt themselves. Every 3rd Sunday for the last 17 years, since I was a GP trainee myself, I have met with Mel Sayer (who is here today) and a small group of other GPs for a study group session lasting 3 hours, including dinner. Undoubtedly, it is because of the support we get from the group, that we are able to be here today.
The Emotional Labour of Care Blog post
Therapeutic nihilism is a consequence of hopelessness in the face of chronic pain, chronic anxiety, loneliness, and complex social issues. Low levels of patient engagement in health promotion and chronic disease management, frequent DNAs and presentations in crisis make matters worse. Therapeutic nihilism It is highly prevalent among GPs in deprived areas and trainees pick up on this. I remember my own naïve therapeutic optimism as a trainee, eager to try new drugs for chronic pain and keen to refer patients with chronic anxiety for EMDR. Therapeutic realism takes time. I’ve given a workshop recently, inspired by Mel Sayer, about doctors and their favourite patients. The longer doctors have known their patients, the more likely they are to be people whose problems have seemed intractable, with whom relations have been difficult. For trainees and younger doctors, favourite patients are those who’s problems they can solve, who are grateful and articulate. Therapeutic realism comes from respect, from doctors ‘standing in awe at the burden the poor have to carry, rather than in judgement at the way they carry it’.
So lesson 1: Poverty medicine is emotional labour
We should let our trainees know that the patients that challenge them most to begin with, might become their favourites, given time and continuity, but feelings of hopelessness and frustration are normal. Being professionally connected to your peers is essential, find or set up a study group and meet regularly.
Lesson 2: Poverty medicine is complex
Coping with complexity: Educating for Capability. Sarah Fraser and Trish Greenhalgh BMJ
Medical students are bought up in a culture where questions have a single-best-answer. Junior doctors and GPs work in a culture full of guidelines and protocols. This gives arise to cognitive dissonance because the impression this creates is that there are much clearer relationships between causes and effects than there are in practice. Teaching the difference between complex and complicated can help us cope with this dissonance.
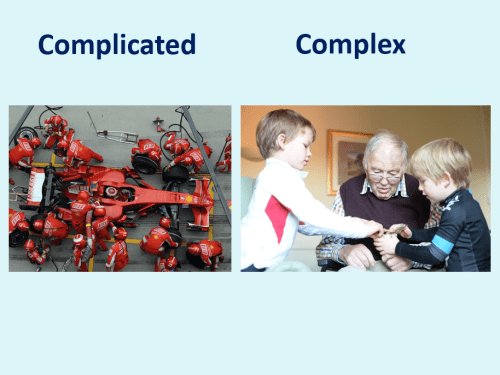
A racing car may be incredibly complicated, but if you can find out which parts need fixing, you can get it running again. Different specialists can focus on the tyres, engine, electronics and so on. We like to imagine people are like racing cars, but they are not, they are complex. My dad is complex. He has cerebrovascular disease and Alzheimer’s, Type 2 diabetes, hypertension, prostate cancer and ischaemic heart disease. Some days he is barely conscious; he cannot eat or drink or get out of bed. We don’t know why this happens. We don’t know when that happens, if he will never wake up again, or whether he’ll be up and smiling the next day, as he is in this picture. One thing that made a difference was stopping all his medication apart from the ones that help him pee. There was nothing sedative in his cocktail of 6 different pills. The medications were stopped 6 months ago. His condition was so poor then, that we thought, even hoped that it might bring his suffering to an end a little quicker with another stroke or a heart attack. But now he’s brighter and happier, and we don’t know how long he might live.
Sandra who I mentioned at the beginning is 25 years younger than my dad. She has 8 different medical conditions. Patients in the most deprived areas typically have the burden of multimorbidity of patients 10-15 years older in the least deprived areas. Sandra is prescribed a total of 16 different medications. She gets a lot of side effects, many of which aren’t mentioned by the BNF. Often she chooses what to take and what to omit based on her symptoms. She owns few clothes that fit her and even fewer that she feels comfortable wearing. She has refused home visits or even to be taken to hospital by ambulance with an exacerbation of COPD because she was too ashamed of her appearance. One of the most effective therapeutic interventions we’ve managed recently was a befriending service. You might reasonably wonder how I’ve defined effective. Well, what I’ve noticed is that when I visit, her skin looks a lot better. Because of the regular visits from the befriender, she’s washing more and using more of her creams for her eczema.
So lesson 2: Medicine is complex, and poverty medicine especially so.
Complex Consultations and the ‘Edge of chaos’ BJGP
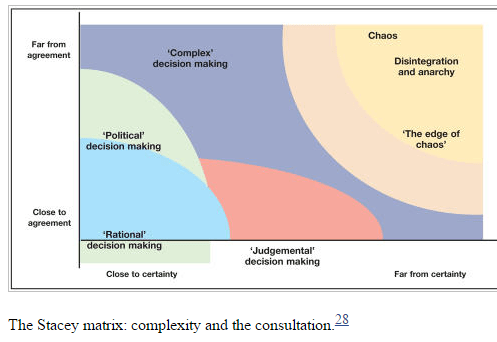
With complexity, relationships between actions and effects are dispositional and patients can be highly sensitive to small changes and respond in unexpected ways.
Dave Snowden: Combining Complexity Theory with Narrative Research
So far, I’ve talked about the problems – Poverty medicine is emotional labour and it’s complex. Doctors, especially stressed, overworked doctors working in deprived areas know this, even if they call it by other names. They want to know what to do about it. It’s easy to suffer from therapeutic nihilism when patients want to discuss chronic pain, chronic anxiety and loneliness and you want to do something about their disastrous glycaemic control.
One thing that has helped me enormously, is by getting a better understanding of patients’ perspectives by reading their narratives. Very often these are written to let us know things they wanted to say, but couldn’t tell us face to face.
Lesson 3: Patient narratives can guide us

I am sure that Julian Tudor Hart wrote this, but cannot find where it was. Very often I find myself having medical discussions with patients and wondering what whether there isn’t something else we would both rather be talking about. Sometimes I have these discussions time and again for years before the ‘real issues’ come out. Trust sometimes takes a very long time to develop.

I teach 2nd year medical students listening skills. By this I mean awareness of how patients’ narratives are created by a dialogic relationship that they have with them. I spend an hour at a time with one patient and 4 students, we watch each-other and take notes about how narratives develop. In their reflective writing about the course, students – almost without exception write about how much they learn from patients.

BMJ What Your Patient is Thinking
Dear Doctor: A letter from a survivor of sexual trauma to all medical professionals
Managing medicines in multimorbidity: a patient perspective
Patients have been writing narratives about suffering illness and receiving care for hundreds of years, and there is a contemporary explosion due to social media. There is a long history of doctors writing, ‘Lessons from the Other Side’ to warn their colleagues that you can complete a medical education and a lifetime in practice and still know almost nothing of what it’s like to be a patient. The British Medical Journal has had an exceptional series of articles called ‘what your patient is thinking’ including the latest one about what it feels like to be an interesting teaching opportunity. Everyone involved in medical education should read this. The first article in the BMJ series was about what it feels like to be a fat patient.
The huge spectrum of responses from clinicians, ranging from fierce criticism to deep sympathy is itself very useful teaching material. Not long before that was published I had published a long, referenced blog called, ‘Doctors, patients and obesity’ exploring what doctors feel when they’re trying to help obese patients. I had written it to help work through my own frustration. I simply didn’t know what to do or how to respond to severely obese patients. I remember discovering how frequently severely obese patients had been sexually abused *ref*. I followed this blog up with essays about how doctors feel about chronic pain, chronic anxiety and lonely patients. All of them were informed by qualitative research and narratives written by patients about how they were treated by doctors. These patient narratives were written, for the most part, not to complain about care, but to help doctors to be more understanding and more compassionate. What patients wanted, but too rarely got, was understanding. One example published this year was ‘A letter to my doctor from a victim of sexual abuse’ in it the author writes,
As a medical professional, you have taken an oath to do no harm, but there are ways in which you can hurt your patients without even recognizing you are doing so. What seems to you as a simple exam may cause injury to those who have been victimized by someone’s touch. This is a subject that we, survivors of sexual violence, have been meaning to discuss with you for some time now, but your authority can be more intimidating than you may know. I am also unsure if you are aware just how much power you, as a physician, hold and to the extent that you affect the lives of all of your patients. Your interactions with us travel much deeper than the physical core.
The young woman who wrote about what it was like to be an interesting teaching opportunity also wanted to emphasise power and powerlessness,
I was asked if some student doctors could observe as they had never seen a chest drain being put in place before. I didn’t feel like I could say no. My situation was being described as ‘a great teaching opportunity’ and was being greeted with a sort of excitement that made me feel uncomfortable. I was starting to feel like the main attraction at some sort of freak show.
One about polypharmacy concluded,
Supportive health professionals, who listen to us and treat us as individuals, are invaluable to people with complicated medical lives. We encounter them far too infrequently. My hope is that clinicians will pay more attention to the complications found in patients’ lives and this will improve outcomes for us all.
I would, of course, say that the right word here is complex, rather than complicated.
So lesson 3: is read, share and discuss patient narratives.
What almost every patient narrative is at pains to emphasise is, “Doctor, I want you to understand what it’s like being me and to know that what you say, the way you behave, and what you do, makes me feel like this.” When Daniel Offri interviewed Oliver Sachs recently she asked him, “Are your patients just much more interesting than the ones we see, do you simply pay more attention to their stories?” Of course, it’s by paying attention to stories that patients become more interesting.
Lesson 4: Adverse Childhood Experiences are fundamental
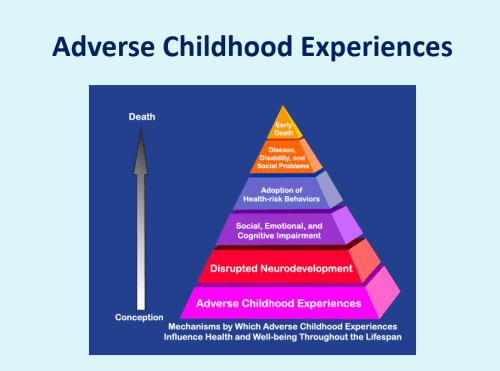
If patient narratives help us make sense of individual experiences, then understanding the effects of Adverse Childhood Experiences helps us make sense of the burden on communities. In the last few months there have been several papers published about the impact of Adverse Childhood experiences, (ACEs) on the future risks of illness and adversity.
Adverse Childhood experiences range from abuse and neglect to living in a household with domestic violence, alcoholism and criminal behaviour. One of the best of these studies is a 38 year cohort study over a thousand children from Dunedin in New Zealand.

The researchers followed up an incredible 95% of the cohort and showed that by 3 years they were able to identify with 80% accuracy those children who were most likely and least likely to be high or low cost in adulthood. High costs were calculated by looking at receipt of welfare, rates of smoking, obesity, hospital stays, prescriptions and criminal convictions. A retrospective study in Wales, published in the Lancet last year showed that 3 or 4 adverse childhood experiences in childhood was associated with a 3 times increased risk of heart disease and respiratory disease and a 4 times increased risk of Type 2 diabetes. Research looking at the effects of deprivation alone, has shown that most deprived 10% of the population have a life expectancy and burden of disease of people 15-20 years older in the least deprived centile and their lifetime healthcare costs exceed the savings incurred by their premature mortality by nearly £5bn.
Part of the frustration that I used to feel with my patients was a reflection of how hopeless and frustrated they felt and a conviction that they ought to be able to do more for their health. I hadn’t appreciated just how much the die was loaded against them at such an early age. Exceptions don’t change the burden of risk any more than someone who smoked all her life without consequences proves that cigarettes aren’t harmful. The burden of adversity in early childhood is associated with far higher rates of harmful behaviour like smoking, alcohol abuse and risky sexual behaviour. An understanding why people behave they way they do is incomplete without knowledge of their experiences right at the beginning of their life.
So lesson 4: Adverse childhood experiences cause lifelong biological damage predisposing to a wide range of diseases above and beyond the psychological harms. They contribute to vicious circles of poverty, unhealthy behaviors and ill-health.
Lesson 5: Understanding the trauma world helps
Daniela Sieff’s website: http://www.danielasieff.com/
The ACE research is at its strongest on demonstrating correlations but is less satisfying at explaining causal factors. Evidence about the long-term effects of stress on neuro-endocrine, cardiovascular and epigenetic systems helps to explain future risks of disease but doesn’t do much to help GPs cope with their primary concern, the patient in front of them. Not everyone who experienced adversity in childhood suffers lifelong harm, but those that do, very often share the psychological and behaviour scars of trauma. Trauma is commonly understood in terms of traumatic experiences or events, such as child abuse or abandonment, domestic violence or even a lack of parental affection because parents were too ill or preoccupied themselves. What has really helped me is the work of Daneila Sieff, who defines trauma in terms of its effects, a ‘trauma world’ that sufferers live in. The trauma world is made up of three areas; fearfulness, shame and disconnection. When I read Sieff’s work and listened to her lecture, it perfectly captured my experience of caring for my most difficult patients. The foundations of a trauma world lie in adverse childhood experiences in which there may be abuse, abandonment or serious lack of affection. When I asked Sandra about this she told me that her parents were in their 40s when she was born, they made it clear to her from an early age, that she was a mistake and so it was mostly down to her sister, who was only 12 when she was born, to bring her up. At 18, her sister died in an accident and the family feel apart, unable to cope with the grief, and she was taken into care.
Fearfulness arises from a fear that the emotions associated with the original trauma will be triggered again. Patients are not usually conscious of the connection and so experience a generalised anxiety about themselves and the world around them. In their relations with us, and other medical professionals they present with the full breadth of anxiety disorders from social phobia to panic attacks and OCD. One consequence of being severely anxious is a tendency to interpret ambiguous social cues negatively, so that sufferers appear highly sensitive, touchy, irritable and hard to engage with, leading to alienation, isolation and loneliness. Because anxiety is so profoundly physical, medically unexplained symptoms are very common. Because deprivation is linked to the burden of disease and multimorbidity, symptoms are very hard for clinicians to ascribe to anxiety on a complex background of vascular, endocrine and neurological disease. And so we too become anxious and stressed.
The second part of the trauma world is shame. Shame is the conviction that what has happened to you and the way you behave is fundamentally because you are a bad person. James Rhodes, whose book, Instrumental is about surviving childhood sexual abuse and finding relief in playing the piano, said,

Shame is the legacy of all abuse. It is the one thing guaranteed to keep us in the dark, and it is the one thing vital to understand if you want to get why abuse victims are so fucked up.
Something you’re embarrassed about makes an entertaining story once you’ve loosened up with a couple of pints, but something you’re ashamed of you do everything you can to hide from others. Patients who feel ashamed avoid eye contact with doctors and fail to attend appointment if they think that they might be humiliated. One of the first pieces of qualitative research I read was Joe Kai’s work in the 1990s on the experiences of mothers bringing sick children to see their GP. They were ordinary mums, a social cross-spectrum. They reported being made to feel foolish for either bringing their children when they weren’t sick enough to warrant the doctor’s attention or leaving it too late and behaving neglectfully. What this, and other similar research has shown is that doctors, consciously or not, so far as patients are concerned, make moral as well as clinical judgements.
Patient reassured. Blogpost about Joe Kai’s research.
The third part of the trauma world is disconnection. Disconnection is the desire to blot out painful memories and emotions. Addiction to drugs that do this, like alcohol, opiates, sleeping tablets and other sedatives is worryingly common. Chronic pain is frequently associated with adverse childhood experiences so doctors prescribe to treat the pain, but the drugs we use – like Pregabalin, Amitriptyline and Codeine are non-selective and numb painful memories as well as back pain. When I met with our local pain clinic director to discuss his clinical approach, he said that he believed in using polypharmacy to block all the pain receptors. I’m not sure that he was talking about the pain of trauma. In a report on anxiety from the Mental Health Foundation it was reported that the second most frequent way that people coped with chronic anxiety was by comfort eating. The US research on Adverse Childhood Experiences began by discovering the strong links between severe obesity and childhood sexual abuse. At first these findings were rejected out of hand by professionals who thought that these were merely patients’ excuses. These attitudes persist today. Sublimation may take other forms of behaviour like burying oneself in work, exercise or shopping, which whilst clearly not diagnostic of a trauma world, might raise suspicions.
The Adverse Childhood Experiences Study — the largest, most important public health study you never heard of — began in an obesity clinic
So lesson 5 is understanding the trauma world can help us to make sense of the overwhelming anxiety, shame and desire for disconnection that our patients suffer.
Lesson 6: Empathy can be taught
The narratives of patients who have written about their experiences of trauma, in order to teach doctors what it’s like, but were too afraid to tell them to their face – share the message that empathy matters, a lot. Empathy is cognitive – the ability to make sense of another person’s perspective and experiences, – and affective – the ability to be emotionally moved by this.
I’m not sure if you can teach someone to feel, but I am convinced that you can teach people to explore and understand other people’s lives. While not every patient will need this, or even welcome it, for best-selling author and Ted Talk celebrity, Brene Brown, empathy is the way we should respond to shame.
The Empathy Exams by Leslie Jamison
For part-time simulated patient in medical student exams, Leslie Jamison, “empathy is asking the questions whose answers need to be told.” Sympathy is a response, “Oh, not, I’m so sorry, that’s awful”. Empathy is a question that shows that actually you have an idea what it’s like, however alien that experience might be. Understanding the role of adverse childhood experiences and trauma offers a framework to guide dialogue.
Empathy demonstrates to patients that they are not alone and that it is possible to make sense of their experiences and that doctors can appreciate what it’s like.
A complimentary perspective about patient’s difficulties in deprived areas, comes from studies of violent behaviour in Scotland. Policeman John Cornachan spent years trying and succeeding to reduce violence between young men in Glasgow. Violence for these men was recreation and whether they ended up in police custody, an A&E department or neither was down to a combination of luck and fighting skills. Violence was recreation for men who hadn’t learned the essential skills of social interaction by other means.
The problems identified by employers weren’t poor numeracy and literacy as we had expected, but, in order of importance: planning and organising, customer handling, problem solving, team working and oral communication. These are skills that are learned and developed in the first five years of life.
Health literacy is a big deal in Poverty Medicine, but while I wouldn’t deny that it is a serious problem, the chaotic lives and serious problems that many of my patients have coping with the bureaucracy of modern healthcare is at least as serious and we could do a lot to make things easier. An over-emphasis on literacy and numeracy means potentially overlooking the need to simplify the ways we provide access to and deliver healthcare.
So lesson 6 is that empathy can be taught – it is created through an active dialogue with patients and is grounded in an understanding of the experiences of deprivation and illness
Lesson 7: Continuity matters

There is a risk that a lecture on poverty medicine deals too little in opportunities. Not every child who has suffered adversity grows up with problems like those I’ve discussed, in many studies, around 30% seen to do OK. Factors that provide resilience include finding meaning and purpose, being able to make sense of experiences and developing a long-term relationship with an emotionally stable adult.
Hilfiker, the Minnesota doctor I quoted earlier understands that a considerable part of his value to his patients is symbolic.
A doctor is more than a set of skills. A doctor is a status, and the presence of that status conveys social inclusion; patients attended by a doctor have not been abandoned.
So lesson 7 is that continuity matters. There’s evidence to show it makes medicine safer, more efficient and more compassionate. And it goes further to promote resilience and inclusivity.
Better continuity of care. Blogpost
Lesson 8: Doctors and patients are in it together
There is a lot more that I could have said and a lot more that GPs could do and trainers could teach. I have another lecture on advocacy for example. But what I wanted to focus on was the experience of being a GP in a deprived community, 8 lessons that I have learned in nearly 20 years of being a full-time GP, that might make up part of a curriculum for poverty medicine and shared with trainees much sooner. The overarching message is that doctors and patients are in it together – what both patients and doctors need is resilience. Harry Burns’ inspiring lecture on inequalities and resilience reminded me of the importance of ‘Salutogenesis’ – the factors that needed to thrive and be healthy, not simply avoid disease and suffering. Antonovsky’s research that showed that to thrive in and after adversity, the social and physical environment must be comprehensible, manageable and meaningful. These lessons have made poverty medicine more comprehensible, meaningful and manageable for me, and I like to think, at least some of my patients, and I hope, some of you too.

Reblogged this on My World, Your World, One World and commented:
Compulsory reading for anyone who says they are concerned for others, about general practice medicine, but so much applies to living, and living well.
Thank you. I reblogged your post. I value so many of the links in it too, working through them now.
Thanks very much, I’ve added some links to the beginning going into some of the things I struggled with in my appraisal, Jonathon
Very well written. Thanks. Working in a GP surgery as a ‘social prescriber’ it summarises a lot of my day to day work.
Wow
I am participating in an on line course on psychology, purely out of interest as I am a retired psychiatric nurse, the article, Working in a GP surgery as a “social prescriber” was posted link by another participant, it has given a much more realistic view of the realities of mental health care than the course.
Reblogged this on Musings of a Penpusher and commented:
This should be compulsory reading – especially for all such as Theresa May who constantly meddle in things they know so little about.
Thank you for such a comprehensive piece, I kept seeing parallels to those of us who offer talking therapies, and how we are failing some of those in the most need.
Thanks Karen. I’m thinking about how attention to salutogenesis might change the way we practice and have in mind health-trainers so that when someone comes in to see a GP and is diagnosed with diabetes or hypertension or depression we recognise it a symptom of a life lived in a particular context and then they can meet – at the practice, there and then – or at a time of their choosing, with the health-trainer who will help them to identify what they need and what they can do to improve things.
Another excellent piece, thank you. I would whole-heartedly support more ‘Poverty Medicine’ in GP training. This is the kind of work I thrive on, but as a young GP it saddens me that modern General Practice does not seem set up to accommodate this.
What advice do you have regarding how to incorporate these lessons into a 10 minute time frame? Regularly scheduled appointments weekly to discuss issues bit by bit? Extended appointments? And with reduced GP numbers, amongst the multitude of others reasons for the breakdown of continuity (practices run by locums/part time GPs/too few appointments), how can GPs best help when it may be near impossible for the patient to see the same doctor more than once?
First is to properly identify the patients’ needs. We’re so problem/solution focused, for years I didn’t really get this. It’s not fair on patients who cannot see us if we see the same small cohort every week, so that’s not sustainable. I think the future is integrating health trainers – e.g. http://www.tandfonline.com/doi/pdf/10.1080/17571472.2012.11493350
Another excellent journey through the complexities of people’s lives and some thoughts about where we, as doctors, can expend our energies to improve health. There are some common threads in primary care and mental health – though recently the interest and focus on providing specific interventions and discharging to GP for mental health services frequently misses the value and need for the ongoing relationship and focus on salutogenesis. I share with our trainees that our jobs are about disease management but equally as important is promoting health and wellbeing – having one without the other seems futile.Part of my role is now as a fully functional part of a primary care team – this removes the notion of referral, and enables longer term support for the patient and wider team and means there is no threshold to see mental health specialists. I think the value of narrative – both for the individual patient – to help understand their own journey, for the staff to reflect on and to empower both to improve social justice is a critical part of working in the medicine linked to poverty and ACEs.
Thanks for a really excellent synthesis of articles and perspectives.
Thanks Sara,
I share your conviction that human relationships are key, not just between clinicians and patients but also between colleagues. I especially like the idea of working with rather than referring to colleagues. I do wonder whether out of the carnage being reaped on the NHS there might arise some new models of care that are relationship centred. I think Margaret Hannah was onto something in her book which i reviewed here https://abetternhs.net/2014/12/11/what-is-the-nhs-for/
Jonathon