In this episode we catch up with Dr Jonathon Tomlinson, an amazing GP in Hackney. Jonathan fills us in with how he is getting on during the coronavirus crisis. He shares his experience working in a practice in one of the hardest hit areas for coronavirus in the UK (1min 40). He tells me how his team has acted quickly to manage the acute situation but also continues to support the long term conditions for many of his patients in the community.
We talk about some of the many changes in primary care over the last few weeks (5min 40s). These include; phone and video consultations; losing the GP waiting room; sharing clinical decisions and talking more with colleagues. We discuss the effects of coronavirus on those people living in deprivation (10mins 10s) and Jonathon shares some experiences from his practice and his patients (11mins). Jonathan talks about the social determinants of health and the importance of prevention along with all the stuff we are seeing in the media at the moment like PPE (14mins 50s) .
One of the things that GPs can do is advocacy and Jonathon was keen to discuss the work of Dr Rudolf Virchow 1821-1902 (19mins). Virchow is famous for saying that politics is nothing but medicine on a large scale and that our role as doctors is to show the link between social conditions and medical diseases (21mins). Jonathan explains why Virchow’s message is particularly relevant at the moment. We explore the role of a GP in advocacy and coordination of a response to support those who are most in need and vulnerable. We discuss how much our job in primary care should include advocacy on behalf of our patients (26mins) and Jonathon offers some ideas for some steps clinicians can take forward to achieve this. Jonathon mentions collaboration, networks (e.g. The Deep End Network), treating long term conditions. We finish our conversation talking about the importance of caring for our patients (28m 55s), Jonathon shares his favourite book (32m 10s), and he tells us what his magic genie wish would be (34m 40s).
We came dangerously close to touching one-another when we came through the door into my consulting room. I held it open for her so she would not have to touch the handle. She held it open with her left foot just as I let go with my outstretched right hand. I had placed our chairs three meters apart, and we sat down facing one another. I sat with my back to the window which meant that her face was lit by the sun while mine was masked by the shade. It wasn’t a deliberate ploy to expose and conceal, but we noticed it as soon as we looked up at one another. I apologised as she winced in the light and I moved my chair around 90 degrees. Fortunately my room is big enough but I’ve consulted in rooms where social distancing is impossible. Everything felt awkward. Consulting has barely changed in hundreds of years. Illustrations of doctors and patients show them sat down at a distance of two to three feet from one another, sat across a desk, or besides a bed. We barely have to leave our seats to inspect our patients. A stethoscope is the perfect length to stretch across the arms-length divide between us. We can inspect hands for signs of disease or reach over to hold them in comfort or pass a tissue to catch the tears. I have spent the last 20 years working at this distance, learning how to judge how much touch is appropriate, and how to ‘harvest the richness of multisensory exposure’ in order to unpack ‘heartaches’, ‘headaches’, ‘bellyaches’ and more.
I am working in uncharted territories without a map. There are technical guides in abundance, but nothing about the relational aspects of consultations where we are separated by physical distance and fear of contagion.
Henri Cartier-Bresson favoured a 50mm lens for his photography because it was the closest to the natural field of view of a human eye. At three meters distance this takes in a full seated figure from head to toe. At two to three feet apart, the way we used to consult, this field of view takes in only a face.
Seated three meters apart we were both aware of how our bodies were exposed to one-another and we wriggled around trying to find a comfortable position. It felt more like a film set than a clinical consultation. There was no desk or computer screen between us. My PPE: mask, gloves, goggles and apron make me feel ridiculous. I peeled off my gloves and apron and I was about to take off my mask, but the sink in which I needed to wash my hands was just behind my patient. We circled each other awkwardly like cowardly boxers in a ring, before taking turns to wash our hands. We sat down again and looked at each-other once more before removing our masks. I took mine off quickly, snapping the straps sharply while she struggled to tear the straps and ended up slipping it down around her neck.
We wanted to go back to the old ways.
Video
I gazed at myself on the computer screen. I moved backwards and forwards, turned my head slightly left and right, lifted my chin up a little, down a little, moved the webcam left and right. I moved the curtains behind me to one side and a picture on the wall across a few centimetres. I turned the lights down and opened the curtains to let in just the right amount of natural light. In the old days I could finish a surgery and then catch sight of some extravagant nostril hairs, a fuzzball of hair that had been blow-dried on the cycle-ride to work, or a stain on my shirt that a dozen or more patients had stared at all morning. These days I’m seeing what they’re seeing, And the critical self-regard is relentless.
My patients have refused a home visit when they were seriously sick because they hadn’t showered or tidied their flat. They want time to prepare themselves before the doctor lays his judgemental eyes upon them. The clinical gaze is full of moral judgement whether it is intended or not. Look too good and the doctor might not take your symptoms seriously enough, look too bad and they might look disgusted. This Goldilocks zone can be precariously small if you’ve been made to feel you got it wrong before. Using the video consultation software lets us see ourselves as others see us and if we don’t like what we see, we imagine they think the same.
Suddenly my patient appears on the screen besides me. I look at her and smile, but catch sight of my face … and my eyes are focused …. where exactly? If I look at her then I am gazing off to the left, if I look at the camera then it looks as if I am looking at her, but I’m not. If I look at myself (I can’t help it) then I’m looking somewhere else. The concentration required is unnatural and exhausting. She was sitting cross-legged on the floor with the phone placed in front of her. She wants to show me where it hurts and it is easier to do that this way. Yesterday someone wanted to show me a rash on their abdomen and they thrust their phone right up against it. It felt like they had grabbed me by the scruff of the neck and held my face inches away from their waist. I physically recoiled from the monitor, but the image stayed the same, wobbling around, in and out of focus.
She clutched her abdomen to show me where it hurt, could it be her liver she wanted to know, I wanted to answer the same way – by pointing to my own body, but my carefully curated head-shot meant I couldn’t get enough of my body in the field of view. She cocked her head trying to see what I was trying to show her as I fiddled with the camera and stood back and up on the tips of my toes and eventually climbed on my chair. In the old days it was much easier to show (and feel) where it hurt.
“Show me where it hurts”
I have felt uncomfortable asking patients to reveal their bodies on a video link. In the old days, patients could undress behind a screen and I would wait until they were ready, or I would lift their vest to feel their abdomen, or guide the patient into the correct position to examine an intimate part of their body. When I visited patients at home people knew that the doctor was there, and you weren’t afraid that someone might burst into the room. I am sure that the awkwardness of examining bodies by video is felt by doctors and patients.
We are amateurs – like clumsy teenage lovers trying to work out where to start. The technology wasn’t made for this; we weren’t made for this. I am a fan of professional Youtubers Contrapoints and Philosophy Tube and have watched them progress from badly lit monologues into set pieces of performance art. In the old days I liked to imagine good consultations like performance art with my consulting room as the backdrop to a drama performed by patient and doctor improvising with one another. Now I have been evicted from my room to make space for a Hot Hub to see patients with suspected Covid-19 and I am working in a minor surgery suite with a telephone and a webcam perched on top of my computer screen. I see only two or 3 patients a day, one by video, one in my new room and one home visit. My normal complex patients with chronic pain, chronic fatigue, chronic anxiety and complex trauma have largely disappeared from my appointment lists, but I have been calling them to see how they are. Paul Dieppe and Julian Tudor Hart wrote a paper in 1996 called Caring Effects showing how continuing interest and ‘caring about’ as well as ‘caring for’ for patients with chronic pain, reduced symptoms, disability, and analgesic medication use.
For some doctors and some patients I am sure that the new world is a welcome relief from the intensity of physical proximity. In interactions with people who present in existential distress/chronic pain most of the effort clinicians undertake is NOT to listen, not to get absorbed into this black hole of despair. Multi-sensory exposure at close proximity is the situation in which they want to press the button for the ejection seat, or for the trap door under the seat of the patient. When doctors give out these ‘not wanting to be there’ vibes, patients, who are often highly attuned to rejection, pick up on them acutely and the desire to escape is mutual.
Little is known about patients’ experiences of these new ways of consulting. Doubtless it’s good for some. But others have complained about the costs, especially people with pay as you go phone contracts. It isn’t suited to people without phones, people who don’t speak English, elderly patients, people without a quiet space to talk, people with sensory impairment, people who struggle to make themselves understood, people who don’t feel safe at home, people who like to be greeted by a friendly, familiar face, people who are isolated and need a reason to leave their homes.
In a face to face consultation spaces between doctor and patient are tacitly negotiated. Access to bodies by way of a physical examination; access to biology with scans and blood tests; and access to life stories; cannot (or at least should not) be taken for granted. Sometimes permission is given explicitly, for example consent to an intimate examination, but usually doctors explore and patients reveal only so far as they feel comfortable. Consent is gradually conceded (or withdrawn) according to how comfortable they feel, which in turn depends on body language – which is lost when we are not together.
A GP surgery and a doctor’s consulting room are physical spaces where secrets are confessed, mortality contemplated, bodies exposed and biographies unearthed. We call this clinical practice, but in many ways it resembles what happens in a church. People go to church or to the GP in order to think, say and do things they do not want to do or cannot do elsewhere. It is about a safe and symbolic space as well as the people in it. I do not think we can do without consulting rooms any more than we can do without churches.
In the old days, I would meet patients in the waiting room, watch them walk towards me and then accompany them to my room. At the end of the consultation I would sometimes walk them back again. Where they waited and how they walked were details that mattered. But nowadays they appear from nowhere and disappear in an instant. In the waiting room I would see other patients, other doctors and nurses and receptionists. I could sense the mood. Walking around the practice I would meet with colleagues and we would talk about patients we were worried about and stuff going on in our own lives. A lot of problems were solved and support given and received in these chance encounters. Now when we come out of our rooms we move as if surrounded by invisible Zorbs. We pass one another with our backs to the wall, holding our breath. We have more formal catch-ups, which is good for some problems but less suited to others. Patients frequently had chance encounters in the waiting room where gossip was shared and friendships rekindled.
Being with and being around people is as important as talking. When my dad died what my mum missed most of all was his presence. He hadn’t spoken much for a couple of years, but she missed his being more than his words. We all miss our patients being around. Many of our receptionists have been in the practice for years and have very fond relationships with our patients: the poppets and the pains in the arse. We’re doing well under the circumstances, but there is an air of sadness. The loading of intimacy with fear fills me with sadness.
Some things we can be sure about. We are novices but we are resourceful and we are learning fast and we will get better. We will be able to offer patients a choice of initial contact- online, by phone or by video or face to face. Many, quite likely most problems can be solved safely and satisfactorily without a face to face consultation. This way patients and clinicians will be free to spend more time with one another when they really need to. It will be especially valuable in hospitals saving patients the trouble of arduous travel, expensive parking and long waits. More clinicians will be able to work flexibly (from home if they want). There will be less waiting and waiting rooms can be requisitioned for social activities – a purpose they served before, even if it was not explicitly acknowledged. But no matter how long this lock-down and fear of contagion continues we will not lose our desire to be with one another.
In 2009 during the H1N1 flu, a public health consultant came to our practice and described a potential situation so utterly catastrophic that we sunk into a collective state of hopelessness and despair for several days. We blocked out any thoughts of pandemics from then on.
Friday 13th I called a consultant foot surgeon about a patient I was worried about. He said that all his clinics had been cancelled until further notice. I asked him what he was going to do. “Play golf!” he replied cheerfully. Now I like to imagine him redeployed to assist nurses in intensive care for 13 hours a day.
That same day I emailed my sons’ cycling club to suggest they called off the session the following day but they replied to say that they were going to carry on, in line with government guidance. Cheltenham festival was still going ahead after all. It was a harbinger of what was to come. That hard choice between following government guidance or doing your own thing. When you’re dealing with large groups of people – 140 kids in a cycle club or 52 employees split across 2 GP surgeries, you need clear guidelines and operating procedures. And where there is usually just one government guideline there are a multitude of feasible alternatives and a consensus can be hard to find.
Saturday 14th Our next-door neighbour told us that a teacher from our son’s school whose son had been staying over with her children and ours a few days before, had been diagnosed with coronavirus. We looked at our snotty children and thought about the number of times we had kissed them in the last 24 hours and realised that it would be impossible to avoid catching it ourselves.
Sunday 15th In the evening after work I felt vaguely unwell with chest tightness, sore glands and a cough. I couldn’t tell if it was psychosomatic. I’m a poor diagnostician when it comes to my own symptoms. A few years before my psychosomatic illness turned out to be an appendix abscess. I called work to say I planned to stay at home for a week. For the sake of my colleagues and my patients it was better to err on the side of caution.
Monday 16th I arranged to stay in touch with my two trainee GPs by phone and video. One called me at lunchtime about a man in his early 60s who worked as a hospital porter. His wife had called because she was worried about him; he was tired, nauseous and couldn’t get out of bed. No cough, no fever, no chest pain, no past medical history, not on any medication, hardly ever gets sick. I suggested that my trainee ask if he, or rather, his wife, would be happy to postpone a visit but have a follow up phone call the following day. When she called back, his wife was in a state of panic – “Come now! He’s going blue!!” The paramedic arrived at the same as my trainee, seconds after he had a cardiac arrest. They tried to resuscitate him with several rounds of CPR but he didn’t survive. My trainee didn’t even have time to put on any protective equipment. We couldn’t prove that he died because of coronavirus but we couldn’t put the possibility out of our minds.
Since then we’ve learned from personal experience and published data, that men in their late 50s and 60s are dying disproportionately and that sudden deterioration at around day 10 of the illness, with an acute worsening of fatigue is an ominous sign. Half my colleagues are men in their 50s. Many of them, because of their experience, are offering to help in the most hazardous places.
Conversations about the end of life
Last week I spend two days calling my most vulnerable patients and their carers to discuss what they would want if they caught Coronavirus and were sick enough to need hospital treatment. Some of them know what it is like to survive a cardiac arrest and ventilation and some of them would be willing to go through it again. If you are relatively well to begin with oxygen therapy might be all you need, but most people understood that the chance of surviving a cardiac arrest bought on by infection with coronavirus in an already frail body would be negligible. “I’ve had my life doc, let them save their ventilators for people younger than me”, said one woman, who is not much older than I am. If I had overwhelming infection and multiple organ failure I wouldn’t want or even expect my colleagues to try to resuscitate me. Not only would my chance of survival with any quality of life be unacceptably low, but the risk of infecting those treating me would be unacceptably high. We are supposed to have the right to refuse any reasonable treatment, but the problem is that CPR is so often performed when it is completely unreasonable, in people whose hearts have stopped because their bodies are too weak for their hearts to keep going. The refusal of CPR is a reminder to professionals whose reflexes are trained to save lives first and think later, that a peaceful death is possible and preferable.
Some of my patients wouldn’t want to go to hospital under any circumstances. We talked about what critical care might involve – oxygen might be enough. Home treatment with oxygen might be an option, but not just yet. For sons and daughters caring for elderly parents, the greatest worry was who would care for their parents if they themselves got sick. I put a note ‘Patient themselves providing care’ on their records to alert anyone that might treat them in an emergency. I promised to help anyone who chose to die at home.
I’ve never experienced so much gratitude as I did in those 2 days of conversations about serious illness and care at the end of life. It helped enormously that we had nearly 20 years of continuity of care before we talked.
Poverty and inequality
We serve a relatively young, deprived, multi-ethnic population in Hoxton in London’s East End. People in their 50s suffer a burden of diseases like heart disease, lung disease, obesity, diabetes and cancer, that people in wealthier areas don’t experience until they are in their 70s. All of these increase their risk of dying from Coronavirus. Lockdown hits them harder too. Childhood poverty is around 40%, twice the average for England and deprivation for older people is more than three times the national average. Many of my patients work as carers, cleaners, on public transport or on checkouts, shop floors, bars, cafes and warehouses.
In the last month we (my family and I) have been fortunate enough to distract and soothe ourselves by baking, gardening and exercising in the forest or in the garden and streaming movies. Life is different for most of my patients.
Isolation and overcrowding
I look after a family with four children between the ages of 3 and 16 and two adults in a two bedroom, 5th floor flat. One of the children is disabled and autistic, one of the adults is addicted to heroin and alcohol. There are countless variations on this theme of overcrowding, disability, mental illness and addiction.
Violence and abuse
Up to 10% of my appointments used to be spent with people suffering anxiety and chronic pain and for many of them it was related to living in fear. A trip to the doctor was an excuse to come to a place of safety and spend time with someone kind and attentive. We didn’t need to (and often couldn’t) talk about what was going on home. I haven’t seen any of these women in weeks. I haven’t had any reports to complete for social services about children at risk. I don’t know if they have safe places to go, or if anyone is looking out for them if they’re not seeing anyone outside the family home.
Digital hardware and data (streaming/ video/ phone-calls/ internet)
At home we’re online all the time. We pay for unlimited wi-fi. But many of my patients are on pay-as you go data contracts and regularly use up their data just waiting for calls to be answered, never mind Netflix. Some cannot use a smartphone or a computer. Some are illiterate. Some of them run up huge debts with multiple phone contracts. Video consultations with your GP are now commonplace, but the more I do, the more I worry about the people we’re not hearing from.
Bulk buying without a car/ money
We are very well served with local shops where I live in Leytonstone and can get all the fresh produce we want. But supermarkets are being stripped bare of essential produce by people whose cars and wallets are big enough, leaving only scraps for people who live one day or one week at a time, who have to walk and carry everything home. They need to get out more frequently, walk the streets and wait in queues.
Access to green spaces
At the weekend I rode my mountain bike in Epping Forest at sundown. It was beautiful and social distancing was easy. My sons played on the grassy flats at the end of our road. We cooked a barbeque in the garden. At work I spoke to a woman with a eight year-old daughter who has ADHD and anxiety. They live on a 8th floor, north facing flat without a balcony. If they want to go out they have to take a lift or walk down a narrow stair case where social distancing is impossible. Victoria Park, the biggest park in Hackney, has been locked shut for weeks because of adults hanging out in crowds. I know parents with young kids who have barely been outside for a month.
Physical distancing
I cycle 9-10km to work every day. It’s easy to keep my distance and stay fit. I have a job that I enjoy, that pays well where I am surrounded by supportive colleagues. We moved rapidly to a mixture of telephone and video consultations and home working, physically isolating ourselves from our patients.
Many of my patients work in jobs that demand travel and human contact –they are carers, cleaners, bus-drivers, shop staff, teachers, nurses, midwives and pharmacists. Most of them depend on public transport to get to work. They are having more far more face to face contact than I am having as a GP and while I have all the PPE I need, many of them have little or none. Analysis of location data from US cities shows that the wealthier you are the sooner you are able to isolate and the more likely you are to be able to work from home.
No social contact may preferable if your main concern is contagion, but it is still a basic human need. My sons haven’t hugged me so much in years. They want physical reassurance and closeness, more than explanations or soothing words. When staff have been unable to come into work because they’ve had symptoms or been in contact with someone who has symptoms (none of us have been tested) they have all been desperate to come back and be around their colleagues. Before Covid-19 many of our must vulnerable patients rarely left home except to see their GP or practice nurse. Being physically present with someone with whom you feel safe and cared for is something too many of us take for granted. Cautiously I’ve allowed some of them back. We sit with our masks on at opposite sides of the room. One woman I look after, who has already spent weeks in intensive care two years ago and is on the high-risk shielding register asked me to come around to have lunch with her. Her son died just a few months ago, “You know me doc, I’m not afraid to die”.
Precarious employment
I have friends who work in hotels, building, catering, and others who are musicians and artists who have all lost their jobs. Many of my patients earned too little to save and are now without work or money. They are dependent on universal-credit and the kindness of strangers. They may have enough to eat but you cannot live on food alone. We don’t know how long this will last or what jobs might be there when it’s over.
Social capital
I can depend on friends and family, most of whom are as fortunate as I am, to help me out – practically, financially and emotionally. Like most of us, in our socially divided country, we are surrounded by networks of people whose circumstances are similar. Often, I am the only professional person my patients know.
Meaning and purpose
Working in the NHS – being lauded on the news and being clapped in the streets every Thursday evening and thanked all day is something I’ll never forget. We’re taking risks, but despite the overused analogies of war, it’s in no way the same as being in an actual war-zone with explosions going off and bullets flying by. We’re not dealing with the bodies of children who have been maimed by landmines and we’re not getting shot at on the way home. What we do have, now more than ever, is a sense of meaning and purpose combined with public outpourings of appreciation.
All of this is on a background of 10 years of austerity in which the welfare state has been stripped back and public health funding has been stripped bare. The NHS has barely recovered from the most shambolic re-disorganisation by Andrew Lansley in 2012, followed by 8 more years of underfunding. We have seen a rise in insecure employment, and a massive distraction with Brexit which has fuelled a breakdown in social cohesion and undermined public trust in politicians and experts at a time when we need them more than ever.
How will we recover?
We have learned that the NHS can change very quickly when driven by clinical leadership and patient needs. Resistance to Lansley’s disastrous market-oriented NHS reforms resulted in a backlash of criticism accusing the NHS of being intrinsically resistant to change and indifferent to patient needs. Now it has been found to be fleet-footed when the people that work there can see that that they are serving patients and not political vanity or private profits. We’ve been allowed to decide for ourselves what’s most important. In general practice we have rapidly taken up telephone and video consultations and we have concentrated our efforts on the interventions we know make the biggest difference – proactive care for our most vulnerable patients, immunisations for children, primary and secondary prevention of cardiovascular disease and better diabetic control. We have stopped the arduous and pointless CQC inspections, GP appraisals and NHS health-checks. We are talking to each other more than ever about patients we’re worried about and getting second and third opinions about complex decisions.
In the last month we have become better connected with community organisations than ever before. Far more of our patients depend on social support than will ever depend on medical care. Long may this develop and continue.
Further reading
To protect population health it will be essential to avoid a further period of austerity and the associated reductions in social security and public service spending. Instead we must build a more sustainable and inclusive economy. British Medical Journal 27/04/2020 https://www.bmj.com/content/369/bmj.m1557
A bioethicist at the heart of the Italian coronavirus crisis asks: why won’t we talk about the trade-offs of the lockdown?
The generals repeated the old lie, “Dulce et decorum est, propatria mori!” Sweet and becoming it is, to die for one’s country
“Hippocrates and Galen, are still renowned for their wise and innovative advice on medical matters. When it came to plague, they offered guidance, rendered in Latin as ‘Cito, Longe, Tarde,’ which translates as ‘Leave quickly, go far away and come back slowly.’ When the Black Death swept over much of Asia, Europe and parts of Africa in the mid-1300s, such advice was about as good as it got.” Bought to Life
Some did stay, out of Christian duty, desire for fame or because they got ‘hazard pay’ from local communities. The idea of a social contract didn’t come around until the 19th century.
At the start of the 20th century the American medical code of ethics stated, “when pestilence prevails it’s the physician’s duty to continue ministering to the sick even in peril of their own lives”
In 1912 the language was strengthened to say there was, “an obligation to continue taking care of people who posed a contagious threat even if you were not being paid to do so.” Ethics Talk podcast
But how far should this duty reasonably extend? Doctors are already dying from Coronavirus infections contracted in the course of caring for infected patients. Many, if not the majority, lack the recommended protective equipment.
Doctors have always placed themselves at risk in the course of their work. In 2003-4 I joined Medecins Sans Frontieres (Doctors without Borders) and I accepted a job in North West Afghanistan knowing that there were risks including death, because of ongoing conflict. While I was there some of my colleagues were assassinated very close to where I was working. Since then I have chosen not to go back to work in conflict zones, but other doctors continue to do so. Doctors’ attitudes to personal risk in the line of duty vary considerably.
At one end of the spectrum are those, like David Nott, the war surgeon, who wrote, “I have travelled the world for 25 years in search of trouble. It is a kind of addiction, a pull I find hard to resist. It stems partly from the desire to use my knowledge as a surgeon to help people who are experiencing the worst that humanity can throw at them, and partly from the thrill of just being in those terrible places, of living in a liminal zone where most people have neither been, nor want to go.” Others are risk averse and under the current circumstances are avoiding all clinical contact while their colleagues continue to work in intensive care units with patients who have coronavirus infections.
I find myself somewhere in the middle of the spectrum. In 2003 I was single and in search of adventure and I felt invincible. In 2020 have young children and I feel more mortal.
We all have reasons for where we might find ourselves on the risk-taking spectrum. One is what motivates us. Not all doctors are primarily motivated to take risks by the desire to save lives or help people less fortunate than themselves. The motivation may be extrinsic rewards like money or fame. Other motivations include intrinsic values like caring, social justice or self-sacrifice which may derive from upbringing, life experiences or religion. Caring can be viewed as a positive motivation; for example, someone bought up in a caring environment with positive experiences of care and caring, for whom caring is an integral part of their identity.
The need to care for others and sacrifice oneself may also come from a need to repair something flawed, damaged or shameful about oneself, to compensate for low self-esteem. Growing up in a relationship with parents who made someone feel inadequate may result in these feelings persisting into adulthood. The adult tries to compensate by self-sacrifice and risk taking. The sense of being flawed or ‘bad’ drives the need to ‘do good’ while the risk-taking is driven by a sense of ‘just deserts’.
There is a strong sense of this when listening to the war surgeon David Nott who places himself not just in high risk, but unnecessarily high-risk situations. Risk for him is both euphoric and addictive. He is the archetype of a heroic doctor, putting the lives of his patients above concerns for his own life. We might hope for him to be our surgeon in a life or death situation, but we might feel differently if we worked with him.
Doctors work in teams; with other doctors, nurses and health professionals as well as admin staff. It’s easier and perhaps more comforting to imagine that the patient is their only, or at least primary concern, particularly in relation to a war surgeon. A GP has to care for individual patients as well as their practice population. We have to support widows who are grieving and be sure that all the children registered are fully immunized. As a senior partner in my practice I am responsible for over 26000 patients and 40 members of staff. The more I sacrifice myself in the services on one person the less I am available for others.
Brain surgeon Henry Marsh is another heroic doctor whose concern for his patients described in his book First Do No Harm runs to commandeering hospital beds and over-riding clinical colleagues and an open contempt for hospital managers whose concern is the smooth running of the hospital. From an individual patient perspective, you’d want him on your side, but if you happened to need a hospital bed for something other than neurosurgery you might feel differently.
Obligations to individuals and populations come into conflict all the time in medical practice and the extent to which our sphere of responsibility diminishes with distance varies considerably between doctors and between individualistic and communitarian cultures. We live in an individualistic culture that valorizes heroes. We are conservative; suspicious of foreigners and socialism having voted for Brexit and 10 years of Tory rule. We are looking for heroes to save us from Coronavirus.
For the last week I have been self-isolating – with what feels like a typical cough and cold. I don’t have breathlessness or a fever. There’s no way of knowing if it is a mild case of coronavirus. Under other circumstances I would be at work. Presenteeism – the phenomenon whereby healthcare professionals come to work in a state of ill-health that they would advise their patients to stay at home, is rife. But this might be Coronavirus. As the pandemic unfolds we might reach a situation where medical professionals are more likely to be infected than their patients. Dr Gordon Caldwell a consultant physician in Oban, has written about what should happen if he requires ventilation because of coronavirus infection.
If I survive to be weaned off the ventilator (1 in 5 chance) it would be at the expense of 1 staff member with severe Covid 19 and 3 others infected, who in turn could infect other staff, patients, and their own family and friends. Until someone can counter this argument with a convincing statistical, not emotional, case, I have stated that I am “Do Not Attempt Cardiopulmonary Resuscitation (DNACPR” and “Do Not Intubate and Ventilate (DNIV)”
Hospitals as well as doctors might soon become the hubs for transmission of coronavirus in the UK if we continue to follow Italy’s lead. The hero who remains on deck after all the passengers and crew have left the sinking ship is not suited to the present epidemic. Our present-day heroes will have to relinquish the helm while they isolate themselves to protect their colleagues and their patients. They will have to trust their colleagues to take over. They will have to show that we can carry on without them.
Michael West – an organizational psychologist who leads on compassionate leadership for the NHS recommends that the priorities should be listening to staff, removing obstacles to safe and effective work, and providing for their basic needs: safety, rest, nourishment and connection. The lesson from this is that during this crisis every single one of us, will at some point have to be a new kind of hero.
Posted onFebruary 23, 2020|Comments Off on Trauma informed care in General Practice
“In the mid 1990s the CDC and Kaiser Permanente discovered an exposure that dramatically increased the risk for 7 out of 10 of the leading causes of death in the United States. In high doses it affects brain development, the immune system, hormonal systems, and even the way our DNA is read and transcribed. Folks who are exposed in very high doses have triple the lifetime risk of heart disease and lung cancer and a 20-year difference in life expectancy. And yet, doctors today are not trained in routine screening or treatment. The exposure I’m talking about is not a pesticide or packaging material it’s childhood trauma”.
Nadine Burke Harris
In this blog, I’d like to suggest what routine screening and treatment might look like in primary care/ general practice. In previous blogs I’ve focused on care for individuals, but here I want to describe a population approach.
Childhood trauma (also called ACEs Adverse Childhood Experiences, is a risk factor for disease, and like other risk factors, for example smoking, the greater the exposure, the greater the risks. Maltreatment that begins earlier in life, is more severe and continues for a longer duration is associated with the worst outcomes. The harm is a result of physiological and behavioural changes; what I have recently described as the ‘Trauma World’ also called ‘Toxic stress’. The word ‘trauma’ is often used to refer to this response, rather than the traumatic events. This is what makes trauma traumatic. For example, PTSD often develops after a supportive partner dies, because their partner provided them with enough resilience to cope with the trauma of their past experiences. Trauma is a legacy of emotional hypersensitivity (or the opposite, alexithymia/ numbness), toxic shame, dissociation and harmful coping strategies. Survivors present to GPs with chronic anxiety, recurrent panic attacks, chronic pain and chronic fatigue. They are more likely to suffer from multiple long-term conditions like diabetes, vascular and lung diseases, autoimmune diseases and cancer at younger ages. As well as being at risk of ill-health they are at risk of violence, abuse, homelessness and destitution. They are less likely to have attended for vaccinations or screening for cancer and they are more likely to smoke, drink alcohol excessively and use drugs including potentially hazardous combinations of prescribed drugs.
A GP practice would want to identify people suffering from trauma in order to diagnose diseases early, to prevent them from developing and to provide appropriate social and psychological support.
A GP practice has a list of registered patients (a denominator) and they will know the numbers of people with long-term conditions such as diabetes, hypertension and depression (the numerators), and they will be invited in for regular reviews. It is easy to identify these people because they have a diagnosis. Because ‘trauma’ is not a diagnosis, it is not tested for or documented like other long-term-conditions so we do not yet have a reliable way of identifying patients who have been affected. A recent study found that trying to identify patients by searching their records for evidence of Adverse Childhood Experiences found only about 1% of those they expected to find.
There is a code for ‘History of complex trauma in childhood’ which has only recently been introduced, but despite my interest in the subject, I am yet to use it because I’m not sure that many people would want it in their medical records. They might rightly fear that other clinicians would bring it up uninvited or worry that whatever symptom they sought help for would be blamed on ‘trauma’. A history of trauma may be hidden in the text of a consultation or a hospital letter, but we cannot search the electronic records in this much detail as we can for diagnostic or problem titles. In any case, it is the presence of trauma, rather than a history of adversity that we are trying to identify. So instead of searching for a diagnosis we could include people with symptoms that are suggestive, if not diagnostic of a past history of trauma; problems like chronic anxiety, chronic pain, irritable bowel syndrome, chronic depression, OCD, self-harm, personality disorders, alcoholism, opiate/ benzodiazepine addiction – and I would include anyone on long-term anti-depressant or antipsychotic medication, regular opiate or benzodiazepine prescriptions.
Patients identified this way might represent 10-50% of a GP practice population depending on issues like deprivation and immigration. Having identified patients, they should be invited in for an initial review and if suitable (more on ‘suitability’ below) added to an ‘at risk’ register for continued annual reviews. Many of these patients will be known to be suffering trauma, and some will not. At the initial review both doctor and patient need to agree whether a regular review would be useful. If there is a disagreement, then the patient’s preference is what matters, after all it’s for their benefit. I would caution against assuming that non-attendance is a sign of disagreement, since people whose lives are insecure and full of anxiety often struggle to attend appointments
The review:
Comprehensive
An annual review should be comprehensive so that all the patient’s long-term conditions are reviewed at the same time, so as not to overburden them with appointments. Their lives are usually filled with bureaucracy as it is. I would include:
A co-created problem list.
It’s been enormously helpful for me to look at patient’s records with them and agree on what to call their different conditions and which are active and significant. It’s an opportunity to think about what the prefix ‘chronic’ means when applied to pain, anxiety or depression. I quite often discover that embarrassing problems like incontinence, mentioned years ago have not been bought up since and are not ‘minor, past problems’ but are definitely ‘significant and active’. In my experience, the process of agreeing on this list together helps both patient and clinician to join-the-dots and see how different conditions relate to one another. At this point it is not unusual for childhood trauma to be bought up and discussed in detail or at least acknowledged. This is a good opportunity to explain the purpose of the review.
An important point here is to recognise that significant childhood trauma is a risk factor for a wide range of diseases and the point of the review is to treat them early or prevent them so far as possible. This can help to reassure patients that far from attributing all their symptoms to trauma, we are staying vigilant for the biological consequences of a lifetime of stress in a way that is safe, structured and planned.
Disease identification and prevention
For many people the experience of past trauma leaves them in a state of tension and hyperarousal, so assessing for hypertension, cardiovascular disease and inflammatory diseases such as arthritis and colitis should be included. Screening for cancer, vaccinations for HPV, childhood viruses, hepatitis and flu, sexual and reproductive health are all especially relevant for people with a history of trauma who may, as a result of insecure, chaotic lives have missed out. Because trauma increases the risks of developing disease, they have more to gain from screening than people more fortunate.
Risk factors relating to coping
People who have experienced significant past trauma often resort to coping strategies that in themselves can be harmful: smoking, excessive drinking, illicit drug use, eating disorders, unsafe sex and so on. We should ask about coping strategies and offer support with smoking cessation and alcohol services, sexual and reproductive health and whatever else is required. We should help them find other, less harmful ways of coping.
Social security
One of the most traumatic events that effects my patients who have already experienced trauma is having their benefits stopped after assessment by DWP. Over 90% of them succeed on appeal but have nothing to live on for 6 months or so while waiting for the process. We need benefits advisers to be available to help people when they need it, within GP surgeries. Social security also includes personal safety and many women that I look after with a history of childhood trauma also have ongoing trauma from domestic violence, so we should ask about this – the HARK questionnaire is a useful aid. We can then refer to specialist supportive services. Young people are at risk of gang violence and exploitation and should be offered support.
Mental health
Many patients will already be suffering from diagnosed mental illnesses, but others will have undiagnosed problems like anxiety, panic disorder, OCD and autistic spectrum disorders. Including mental health as part of a general healthcare review helps to create a culture in which a healthy mind and body are considered together.
Medication review
People with a history of significant trauma are often prescribed a lot of drugs to help alleviate their symptoms and treat their various long-term conditions. A medication review is an opportunity to talk about which drugs are helping and which ones are no longer useful and which ones are harmful; to check for side-effects, interactions and risks including dependence and accidental overdose. We have a clinical pharmacist in our practice who can help with medication reviews including tapering regimes for people who want to come off harmful drugs.
Social prescribing and social isolation
One of the consequences of trauma is that survivors are more likely than others to be isolated and lonely. Annual reviews could take the form of ‘group consultations’ already being used successfully for diabetic annual reviews. There could be a social space in the practice, in the waiting room if it is big enough, where people can get a cup of tea and sit around tables where they can chat while waiting to see a clinician. Some people much prefer to be in their own space, so they need to be made to feel safe and comfortable as well. Most practices can refer patients to social prescribing to help patients find safe places to be doing things with other people in the community.
Physical wellbeing
Bottom up therapies are things that you can do to feel more in control of your body. It can be anything from knitting to yoga, from gardening to parkrun. Nerve fibres from the body travel up to the brain, so that things that make our bodies feel capable, controlled and strong also help our minds to feel the same way. For many people this is much more effective (and acceptable) than psychological therapies. Most practices can refer for exercise programmes and some are even introducing other activities like tai chi and therapeutic gardening.
Nutrition
It is hard to be feel well if you are unable to afford to eat well, if your diet is unhealthy or food is associated with shame. Programmes like Food For Life run by Shoreditch trust can help people learn to change their relationship with food https://www.shoreditchtrust.org.uk/health-and-wellbeing/food-for-life/.
Conclusions
This is an idea and not something that I have implemented, yet. From a GP perspective it might seem like a lot of additional work, but I suspect that most people identified will already be coming in for a review because they have previously been diagnosed with other long-term conditions. It will identify new patients by including a new set of long-term conditions like chronic pain and addiction. I hope that it upsets the Bio-psycho-social hierarchy by making social security, mental health and physical health equally important. I hope too, that it helps to reduce the risks of diagnostic overshadowing by taking a proactive approach to the early identification of disease in people at high risk. Most of all I hope that it helps doctors and patients to come to a better shared understanding of one another by co-creating a problem list and thinking about why it looks that way and what the implications are. And from this I hope to shine a light on hope and salutogenesis.
John sat next to his mum, an elderly, anxious looking woman who did most of the talking. He rubbed his palms hard together, as if trying to rub out a stain while she talked. He was sweating and his right leg kept trembling. He clamped his hands between his thighs to keep his leg and hands still. Mostly he looked down, without focusing, at the floor in front of him. He wore a black jacket over a grey tracksuit with white trainers that had seen better days. He was new to the practice, though I had met his mum a few times before. He wasn’t long out of prison and Janet, his mum, had told me a while ago that she wanted to bring him to see me when he got out. Fortunately the recent spell inside had been short and we had a pretty decent set of notes from his previous GP.
Before he came in I looked at his ‘problem’ list. The electronic patient (medical) record (EMR) has a list of Active and Past Problems, sub-categorised into Significant and Minor. A patient’s problem becomes a Problem in the EMR when it is picked up by the EMR and ascribed a code. A Problem can be a diagnosis, a symptom, or anything else a patient reports that a doctor or a medical summariser adds to the record, so long as it is picked up by the EMR (it comes up in blue text as you type it in). Problem codes aren’t (though I would like them to be) a definitive list of a patient’s problems, but they can be useful. John’s problem list ran to about 160 entries over 4 pages. There were Problems that weren’t problems like, ‘Telephone call to patient’ and ‘results discussed’ as well as Past Problems that I suspected should have been Active Problems like, ‘Anxiety’ and ‘Depression’. Some Minor Problems like ‘Alcohol Problem Drinking’ and ‘Overdose of opiates’ I thought were probably Significant. Problem lists accrue over years and if they are not ‘tidied up’ it becomes impossible to see what problems are ‘Active and Significant’ because they are mixed up with everything else. Another issue is that different problem codes are used to refer to the same problem, for example:
Anxiety states (Significant Past)
O/E anxious (Minor Past)
Generalised Anxiety Disorder (Significant Past)
Anxiety NOS (Minor Past)
Anxiety with depression (Significant Active)
Panic attack (Significant Past)
Agoraphobia (Minor Past)
Social Anxiety (Minor Past)
Irritability and anger (Minor Past)
Often the same Problem code is there repeatedly; there were 5 Anxiety States, 4 O/E anxious and 3 Anxiety NOS. as if anxiety is something new each time, rather than a chronic, enduring state.
Problems relating to anxiety were a feature of his problem list from the age of 11 up to his present 41 years.
Other Problems referred to physical symptoms and conditions that frequently accompany anxiety:
Dyspepsia (8 times, Significant Past, 3 times, Minor Past)
Bloating symptom (5 times, Minor Past)
Abdominal pain (5 times, Minor Past)
Chest pain (4 times, Significant Past
Dizziness
Feels Faint
Insomnia
Urinary symptoms (3 times, Minor Past)
Burning symptom
Going through a problem list is like examining a crime scene for evidence in order to make sense of what has gone on. A problem list is limited by culture, assumptions, omissions, misunderstandings and mistakes. It serves as a tool for audit and finance – we need to know how many patients we have with depression/ diabetes/ cancer/ heart disease and so on so that we know can make sure that we call them in at regular intervals for proactive, preventive care and get paid for it. Because of this, certain problems like these are more reliably coded than others. The presence of multiple problem codes referring to anxiety over a lifetime suggest that anxiety isn’t just situational, but has something to do with what happened in childhood or perhaps a genetic/ familial trait. Taken in conjunction with multiple related physical symptoms, the issue looks more like a lifetime of hyper-arousal – a state of chronic fight of flight than of anxiety alone.
One consequence of being stuck in a state of ‘fight of flight’ is exhaustion. This hyper-vigilance is unsustainable. In childhood it comes across as hyperactivity or ADHD, but with increasing age this gives way to exhaustion with chronic fatigue, depression and chronic pain, or cycles that swing from mania or hyperactivity to depression and numbness. I note that John has ‘Emotionally Unstable Personality disorder [replaced Bipolar disorder]’ among his Active Significant Problems. For some people, this chronic stress causes autoimmune diseases like inflammatory bowel disease, connective-tissue disease or inflammatory arthritis.
There were Problems relating to pain:
Abdominal Pain
Generalised pain
Back pain
Low Back Pain
Chronic Low Back Pain
Lumbar Disc Degeneration
Sciatica
Pain in leg
Radiculopathy NOS
Neck pain
Cervicalgia
I looked for Problems that suggested ways of trying to cope with chronic anxiety, depression, exhaustion and pain.
Opiate misuse
Diazepam dependence
Alcohol problem drinking
Self harm
Accidental overdose
Suicide attempt
The problems suggested something that Daniela Seiff wrote about in Understanding and Healing Emotional Trauma called The Trauma World. I’ve adapted it to use in practice – as shown in the slide below. The Fight or Flight response which may include psychological symptoms of anxiety and hyperactivity as well as physical symptoms like irritable bowel syndrome and palpitations comes under hyper-arousal. These are usually the most obvious or visible symptoms. The flip-side, the ‘freeze or flop response’ includes fatigue, alexithymia (numbness) and chronic pain and comes under hypo-arousal. Toxic Shame refers to pervasive self-blame and may include suicidal behaviour and self-neglect. Symptoms like depersonalisation, derealisation, and functional neurological symptoms like non-epileptic seizures are examples of Dissociation. The use of stimulant or sedative drugs – prescribed or illicit, comes under ‘Coping’. According to this model, addiction is a symptom of The Trauma World, not something separate, or even the primary problem. In red I have written words that refer to the experiences that people who live with The Trauma World suffered when their trauma was committed and frequently continue to suffer in their interactions with medical (and other) professionals; cruelty, disbelief, blame and rejection/ chaos.
There are no simple answers to Trauma World, but there is a mirror image that I have found to be useful, which I call The Healing World.
Where there has been cruelty we can be kind, where there has been disbelief, validation, where there has been blame and shame, vindication and where there has been chaos (and rejection) commitment and consistency, demonstrated by continuity of care. The fingers and thumb don’t mirror the Trauma World, but do serve as a guide for what’s needed. Mind refers to feelings, memories and thoughts which can be helped by therapy. Body refers to physical activity which might be yoga, Tai Chi or knitting, singing, dancing or baking. Something where the focus of attention is on doing things controlled and creative and ideally rhythmical with the body. Biology refers to everything that goes in the body – food and drink, even fresh air. It is a reminder that medicines are only a small part of The Healing World and that what you put in your body affects every part of your body. Positive human relationships have been proven to be the most important factor in recovery from trauma. People are often isolated, lonely and frightened of human interaction, afraid of what other people might think of them or say about them. Feelings of shame, anxiety and depression colour interactions with pessimistic expectations; ambiguous social cues are interpreted negatively. This can be so hard to overcome, and may take years and long-term relationships and unconditional love. A friend and survivor of trauma who runs groups for men who were abused reminds me that, “there are too many of us for you [GPs] but you can help us to help ourselves by providing space for us to meet and run peer support groups'”
Social security is absolutely vital. It is why there is The Trauma World has a social gradient; people who are deprived have fewer resources to buffer the effects of trauma and may live with the threats of violence and destitution. Social security wraps around everything else; make a fist and your thumb wraps around your fingers.
With John beside me, we look at his problem list together. One significant and profoundly useful act, is to agree about what Problems are Active and Significant and what labels accurately describe his symptoms. There no Problem codes for “The Trauma World’ or ‘Complex Trauma’ or even ‘Complex PTSD’. There is ‘Other PTSD’ and ‘Chronic Anxiety’, ‘Chronic Depression’ and ‘Chronic Pain’. We add ‘Irritable Bowel Syndrome’ and ‘Irritable Bladder’. After ‘Other PTSD’ I add a note – ‘discussed with patient, see consult 20.01.2020’ If patients are to receive the benefits to which they are entitled, then at the very least they need a medical report that is accurate and has a list of mental health conditions – in John’s case, Generalised Anxiety Disorder, Panic Disorder, Agoraphobia, Complex PTSD, Depression, History of Self Harm and Suicide Attempts. Emotionally Unstable Personalty Disorder may be unacceptably pejorative, but it’s might be of use in a benefits claim.
I don’t know what happened when John was growing up. I’m not at all sure that it’s necessary for me to know. Probably only if and when John wants to bring it up. There’s enough in his Problem list to know that ‘stuff happened’. Usually though, once we’ve worked through the list and seen the pattern, we’ve laid down a foundation for trust and the past comes out. In that case I document it and leave a reference next to the problem title, so that in future another doctor can look it up without John having to go through it all again.
The Trauma World and the Healing World are grounded in patient experiences and clinical practice. They are a call to action. They demand that we take notice of the bigger picture, that we stop making distinctions between mind and body, that we pay attention to shame and injustice and do something to make a difference.
Three and a half weeks ago I crashed my mountain bike riding downhill over a jump in Epping Forest, trying to keep up with my 9 year old who is perfectly comfortable being airbourne. I somersaulted in mid air landing on my back, then bounced onto my head and back onto my back (or something that felt like that). The small backpack I was carrying with tools, snacks and spare tubes, dug into my back on the right side of my chest and I was winded, speechless and in a lot of pain. My ride home was exquisitely painful. I diagnosed myself with 2 fractured ribs at the back of my chest and one at the front on the right side and one at the front on the left – I could feel a small step and some movement where they hurt, and still, sleep is almost impossible, sneezing agony and I cannot find any painkillers that do much (apart from 100mg diclofenac suppositories which give me about 5 hours relative relief)
I went back to work the day after the crash – GP partners have a ‘shadow contract’ which stipulates that we shall continue working up until the point of death and for a minimum of another month after that.
It’s still painful, but I can ride to work (10km) so long as I don’t stand up or change speed too quickly.
I’ve begun to notice small signs of improvement and changes to the nature of the pain. More and more it seems to hurt deep inside – where my liver is. I’ve been telling my (non-medical) wife that my liver feels bruised.
Yesterday a partner came back to work after maternity leave, noticed my discomfort and asked what happened. “How do you know you haven’t got a liver haemorrhage?!” she asked, aghast. I let this sink in while my attention drifted into and around my ache.
Ever since then it’s been impossible to shift the focus of my concern. Now it’s my liver that hurts more than my ribs and the nature has become more of a tense, dull, livery kind of pain and less of a sharp, crunchy ribby kind of pain. I’ve given up alcohol for a month and paracetamol and have started being more cautious with how I move.
Simply being more focused on ‘a bleeding liver’ has changed my pain perception and my pain behaviour. It definitely ‘feels like’ my liver is swollen and engorged with a big blood clot. If I have a scan and can see how much or how little damage there is (as represented by the scan) how will I feel then? If it’s ok, will the pain resolve, will I celebrate with a drink? If not, will I worry more and if it looks bad, will the pain get worse and more ‘livery’?
I don’t know.
The iatrogenic harm (harm done by the things doctors say and do) that comes from a suggestion is significant, but largely overlooked – by doctors at least, except perhaps by GPs who are constantly picking up the pieces after their patients have attended A&E with unexplained symptoms onto which an enthusiastic junior doctor has attached a list of possible diagnoses that their daft old GP couldn’t possible have thought of. Our patients come back to see us saying – “the hospital told me you have to refer me / arrange a scan …” Furthermore the more tests we do, scans/blood tests etc. the more abnormalities will show up that are unrelated to any disease or adverse prognosis, but are a reminder that our bodies are flawed and imperfect. A reminder that may make us actually feel unwell.
By not presenting myself to hospital, but avoiding a scan, I’m avoiding a diagnosis, a label and a cascade of interventions. I’m also evading the potential indignity of poor care and invalidation. I’ve had a lot of A&E and follow up hospital visits in the last year of cycling related trauma and the petty humiliations: being ignored, nobody introducing themselves, being patronised and condescended to, upset me. But also it’s upsetting because I / we are all representatives of the NHS and these petty humiliations are symbolic of a service that is failing. And this is another kind of pain I’m keen to avoid.
If your impression of NHS general practice is one of terminal decline and despair, you’re looking in the wrong places. The wonderful paradox that is General Practice at the Deep End has proven yet again that if you want to be inspired by examples of clinical excellence, educational innovation, and passion for practice then you need to be talking to people delivering primary healthcare to the most vulnerable people in the most challenging places.
Relationship-based care – connecting people and places
Generalist, multidisciplinary primary care
Proactive, anticipatory and planned care
Education, research and advocacy for patients and providers
Biology is bound up with biography. The doctors, nurses, social workers, health-visitors, district nurses and Focused Care Practitioners who work with vulnerable people bear witness to their lives and their stories. Adverse childhood experiences aren’t an abstract notion for professionals who visit their homes, stitch up their wounds and drink tea with people whose lives are beset with trauma we can barely imagine. We make human bonds over time, and develop trust, respect and affection that flows both ways. Our surgeries are safe havens, ‘palaces for the people’ where people who have power and privilege listen and are kind to those who do not, and are capable and use their power to heal and enable. Trusted people and places build connections and create formal and informal networks. People discover that they are worthy of care and attention. There are places where one need not feel ashamed.
Generalist, multidisciplinary primary care
The most vulnerable people – those with learning difficulties, serious mental illnesses, the homeless, abused and addicted – die two or three decades younger than the most fortunate. They die from the complications of under-treated long-term conditions like hypertension, heart-disease, diabetes, asthma and COPD. Treating these conditions can narrow the gap in life-expectancy. But these conditions are ‘silent killers’ because they are usually symptomless. Suffering comes from anxiety and depression and the stress and distress of poverty, hunger, violence and neglect. Where we cannot offer a cure, we provide relief. Holistic, generalist primary care is concerned with the relief of any suffering, no matter what its cause.
Proactive, anticipatory and planned care
Far from the ‘worried well’ that most GPs complain about, and the worried unwell that worry us, the unworried unwell are the ones we are most concerned about. These are the patients who attend when they are in crisis but whose arteries are about to catastrophically thrombose under the stress of uncontrolled hypertension and diabetes. Planned care with routine appointments in pre-arranged clinics doesn’t work well for people whose lives are filled with crises or whose mental health is precarious or who don’t know or don’t care or have other, more pressing concerns. They need anticipatory care – attention to what might kill them, whenever they on attend with what ails them. They need proactive care- delivered at home, in the night shelter, on the streets even, wherever we can track them down. We need to know who our patients are whose health-care needs have been neglected and make sure nobody is omitted.
Education, research and advocacy for patients and providers
We need professionals with the skills suited to the problems that they are expected to deal with; complex multimorbidity with social insecurity, chronic pain, addiction and adverse childhood experiences are highly prevalent and can be distressing for professionals who are not prepared or well supported. We should use research to advocate for political action on the political and economic drivers of inequity, the poor housing, poverty and insecurity that results and the high prevalence of diseases that we have to treat. Failure to act upstream means we need more resources to treat the consequences downstream.
Hope: focus on what is possible
Those of us who work in the Deep End know how bleak the situation is. We don’t go to conferences to be reminded of our daily grind. We go to discover what is possible, to hear from people who are succeeding and thriving despite austerity. Professionals who work in areas of deprivation frequently talk about how much they learn about resilience, survival and recovery from their patients. Just because it’s possible to overcome adverse childhood experiences doesn’t mean that we won’t fight for children’s rights. Just because some poor people can eat well from food banks doesn’t mean that we think that food banks aren’t the result of a profoundly unjust set of policy decisions in the wake of the global financial crisis. Focusing on the possible protects us from nihilism and despair, keeps us open to learning, helps us to seize opportunities, keeps lines of dialogue open. The hopelessness that so often accompanies poverty can be contagious, but so is the hope and optimism that goes with Deep End general practice.
Solidarity: we’re part of a movement
Shared values, a shared mission and an infections optimism bind us together. Contributors at the conference from England, Ireland, Scotland, Wales, the US, Lebanon and Belgium showed us that at the same time as it is possible to be an expert in the health needs and behaviours of people in a specific place it is also possible to be kindred spirits with doctors from all over the world. Doctors in deprived practices are often professionally isolated and heavily burdened by the complexity and emotional labour of care. To bond with peers with whom you are morally and intellectually aligned is empowering and energising.
Thanks to GPs at the Deep End all over the world.
The Exceptional Potential of General Practice – Conference Programme
University of Strathclyde Technology and Innovation Centre, 99 George Street, Glasgow G1 1RD.
Day One: Thursday, 14 February 2019
13.00 Arrival and registration
SESSION ONE: Dr Julian Tudor Hart and The Inverse Care Law
Chair: Dr Carey Lunan, Chair of RCGP Scotland
14.00 Welcome and introduction: Dr Carey Lunan
14.10 The example of Dr Julian Tudor Hart: Professor Graham Watt
14.30 The Inverse Care Law – market forces: Professor Allyson Pollock
14.50 The Inverse Care Law – research evidence: Professor Stewart Mercer
15.10 Discussion
15.25 Break
SESSION TWO: The Exceptional Potential of General Practice
Chair: Dr Carey Lunan, Chair of RCGP Scotland
15.55 Serial encounters: Dr Iona Heath
16.15 Community practice: Dr Peter Cawston
16.35 Big data: Dr John Robson
16.55 Discussion
17.10 Close
Day Two: Friday 15 February 2019, Morning Session
From 08:45 Registration
SESSION THREE: General Practitioners at the Deep End
Chair: Professor Graham Watt, University of Glasgow
09.15 Welcome and introduction
SCOTLAND
09.20 General Practitioners at the Deep End: Dr Anne Mullin
09.30 Govan SHIP: Dr John Montgomery
09.45 The Pioneer Scheme: Dr Petra Sambale
10.00 Discussion
IRELAND
10.15 The Irish Deep End Project: Dr Patrick O’Donnell
10.30 GP training and recruitment: Dr Austin O’Carroll
10.45 Discussion
11.00 Break
ENGLAND
Chair: Dr Helen Stokes-Lampard, Chair of RCGP Council
11.30 Yorkshire/Humber: Dr Elizabeth Walton
11.45 Greater Manchester: Dr John Patterson
12.00 Discussion
PANEL AND PLENARY DISCUSSION
12.15 Where next for the Deep End Projects?
13.00 Lunch
Day Two: Friday 15 February 2019, Afternoon Session
SESSION FOUR: Future Challenges
Chair: Dr Khairat Al-Habbal, Lebanese American University, Beirut
14.00 Welcome and introduction
14.05 Social Medicine: Professor Jan De Maeseneer
14.25 The Wider World: Professor Sir Andy Haines
14.45 The Educational Challenge: Dr David Blane
15.05 Break
SESSION FIVE: What Does the Future Look Like for General Practice?
Moderator: Dr Richard Horton, Editor, The Lancet
15.30 Plenary discussion with panel
16.30 Close
The Exceptional Potential of General Practice
Speaker Biographies
David Blane is an academic General Practitioner at the University of Glasgow and has been involved in the Deep End group since 2010, combining clinical work as a part-time GP with teaching and research commitments. He was awarded a Master of Public Health degree with distinction in 2012 and his PhD in 2018. He has authored several Deep End reports and manage the group’s social media presence. He is Academic Co-ordinator of the Deep End GP Pioneer Scheme.
Peter Cawston is a full-time GP Principal in a Deep End practice and was GP Cluster Quality Lead for seven Deep End GP practices in Drumchapel, Glasgow, Scotland. He qualified in Glasgow in 1993 and after working in France for two years completed GP training and a GP higher professional fellowship in Glasgow, where he has now served as a Deep End GP since 1999. Other roles have included: clinical lecturer, working with several patient groups and leading the Scottish Government’s pilot Link Worker Programme. “The mainstay of my working life, however, have been the long term relationships with colleagues in my practice team and with our patients on whose trust, forgiveness, good humour and resilience we rely every day.”
Jan De Maeseneer chaired the Department of Family Medicine and Primary Health Care at Ghent University from 1991-2017. He contributed to the development of inter-professional Community Health Centres in Belgium, with integrated needs-based capitation financing. His research focused on equity in health, strengthening PHC and improving social accountability. He chaired the European Forum for Primary Care from 2005-2017 and was Secretary General of The Network: Towards Unity For Health from 2007-2015. He chairs the Expert Panel on Effective Ways of Investing in Health, advising the European Commission.
John Frey qualified in medicine in 1970 from North Western University, Chicago. When he worked with Julian Tudor Hart in South Wales in the early 1970s he was the first family medicine-trained US doctor to work in the British NHS. He was head of the Department of Family Medicine at the University of Wisconsin, Madison for 13 years. Now retired, he remains active and is a regular contributor to the BJGP on US health care issues.
Andy Haines was Dean (subsequently Director) of the London School of Hygiene & Tropical Medicine for nearly 10 years until October 2010 and is currently Professor of Environmental Change and Public Health. He was a family doctor in inner London for many years and formerly Professor of Primary Health Care at UCL. He has been a member of many national and international committees, including the UN IPCC, and was chair of the Rockefeller Foundation /Lancet Commission on Planetary Health. His research interests focus on the linkages between health and environmental change including sustainable healthy cities and food systems.
Iona Heath, General Practitioner at Kentish Town, London for 35 years, and Past-President of the RCGP, has written regularly for the British Medical Journal and has contributed essays to many other medical journals across the world. She has been particularly interested to explore the nature of general practice, the importance of medical generalism, issues of justice and liberty in relation to health care, the corrosive influence of the medical
industrial complex and the commercialisation of medicine, and the challenges posed by disease-mongering, the care of the dying and violence within families.
Stewart Mercer is an academic General Practitioner, having worked clinically in a range of settings including the Deep End. He was a researcher at Glasgow University for 20 years studying inequalities in health and health care and the importance of empathic, patient-centred care. Since 2008 he has led a programme of research on the needs of patients with multiple complex problems (multimorbidity). He has expertise in the development and evaluation of complex interventions and has been the Director of the Scottish School of Primary Care since 2014. In 2019 he is moving to a chair at the University of Edinburgh.
John Montgomery has worked in the David Elder Medical Practice, Govan Health Centre since 1987, initially as a registrar, as a partner since 1989 and now as senior partner. He became a GP trainer, developed an interest in diabetes with the SCI Diabetes Group, had a spell in medical broadcasting with BBC Radio Scotland, was elected chair of the South Glasgow GP Committee and now has the Lead Clinician role in the development of the Govan SHIP project.
Anne Mullin has worked in Govan for 24 years as a GP and “I am exactly where I want to be in my career”. She chairs the Steering Group of General Practitioners at the Deep End.
Austin O’Carroll, General Practitioner in Dublin, founded several initiatives addressing health inequities: Safetynet primary-care service for over 6000 marginalized patients annually; GMQ, primary-care service for homeless people; Partnership for Health Equity, a research, education, policy and service delivery collaboration; Curam Healthnet, creating new GP practices in areas of deprivation; and the North Dublin City GP Training programme. He completed a Doctorate in ethnographic research into the health service usage behaviours of homeless people. He received the Irish Health Professional of the Year Award in 2015.
Patrick O’Donnell graduated from a rural vocational training scheme in 2012, competed a master’s degree in global health and now works as a GP and Clinical Fellow in Social Inclusion at the University of Limerick. He is currently doing a PhD on social exclusion and primary healthcare. As well as working as a GP in a disadvantaged area of Limerick city, he runs clinics for marginalised groups who do not have access to mainstream medical care.
John Patterson is a General Practitioner and Medical Director of Hope Citadel Healthcare, a NHS Social Enterprise running nine practices covering 31,000 patients in hard-pressed neighbourhoods around Greater Manchester. Their response to the demands of the ‘Deep End’ was to design a ‘Focused Care’ model to bias healthcare access to the most vulnerable and needy households. Three of their practices have been rated ‘Outstanding’ by CQC. From 2018 he was appointed CCO of Oldham CCG.
Allyson Pollock is Professor and Director of the Institute of Health & Society at Newcastle University. A public health physician, she is a leading authority on the fundamental principles of universal health systems, marketisation and public private partnerships, and international trade law and health. Her current research is around access to medicines, pharmaceutical regulation, and public health; and child and sports injury. Her book NHS plc: the privatisation of our health care was published by Verso, and she is currently working on a book An Anthem for the NHS.
John Robson has been a GP in Tower Hamlets, East London for 37 years, has a longstanding interest in cardiovascular disease, chaired the NICE guideline 2008 on lipids and CVD risk estimation and was a co-author of the QRisk and QDiabetes scores. He is CV lead for University College London Partners and Tower Hamlets CCG and Clinical Effectiveness Group lead at Queen Margaret University London (QMUL). He has carried out a range of research studies on the evaluation of quality improvement in equitable health service delivery.
Petra Sambale has worked in both the UK and her native country Germany. She qualified as a GP in Glasgow and has been a partner in Keppoch Medical Practice since 2000. She values the principles of the NHS and enjoys being a GP trainer in an area of concentrated deprivation. She believes GPs have an important part in addressing health inequalities. Her involvement in the Deep End Steering Group led to her current role as Lead GP of the Deep End Pioneer Project.
Elizabeth Walton is a Clinical Lecturer in primary care medicine and a GP in the most deprived area of Sheffield at the Whitehouse Surgery. Her NIHR funding is to develop research and teaching skills with a focus on health inequalities. Her passion to work towards health equity for communities and to support professionals working with vulnerable groups was inspired through witnessing the contrasts in the social determinants of health for patients throughout her career.
Graham Watt is an Aberdeen medical graduate and after hospital jobs in Shetland, Leicester, Aberdeen and Nottingham worked as MRC Research Registrar at Glyncorrrwg in South Wales with Julian Tudor Hart. After GP training at Ladywell Medical Centre in Edinburgh and Townhead Health Centre in Glasgow, he completed public health training with posts in epidemiology, health services research management and academic public health. Despite this circuitous route, he had the great good fortune in 1994 to become Norie Miller Professor of General Practice at the University of Glasgow. He retired in 2016 and is now Emeritus Professor.
Chair Biographies
Khairat Al Habbal is a family medicine specialist in Beirut and Clinical Instructor of Family Medicine and Social Medicine at the Lebanese American University, Beirut .
Richard Horton graduated in medicine from the University of Birmingham in 1986. Since 1995 he has been Editor-in-Chief of The Lancet.
Mayur Lakhani is President of the Royal College of General Practitioners and a General Practitioner in Sileby, Leicestershire.
Carey Lunan is a GP at Craigmillar Health Centre in Edinburgh and is Chair of RCGP Scotland.
Andrew Lyon, after working in shops and factories, studied Sociology and Economics at Edinburgh University. With the International Futures Forum, he worked to restore effectiveness in times of rapid change. He chaired the Deep End Steering group from 2009-16.
Helen Stokes-Lampard is Chair of the Royal College of General Practitioners and a General Practitioner in Lichfield, Staffordshire.
Four patients in my afternoon surgery were suffering from chronic pain and had spent years being treated by pain specialists, spinal surgeons, psychologists, physiotherapists and complementary therapists. None of this specialist attention had alleviated their pain to any significant degree or provided a satisfactory explanation for their suffering. I have long-since stopped trying to ‘explain pain’, but for people who want explanations there are excellent resources online like ‘Pain is Weird’ by Paul Ingraham on Painscience.com and Tame The Beast by Professor of pain science, Lorimer Moseley.
Two of these patients with chronic pain had suffered child sexual abuse and one had also been a child slave. One had been tortured by the police in his home country and one had been traumatised by having to kill people when he was an army conscript. One of the women who had been abused had been seeing me with her back pain for 13 years and yet I only learned a few weeks ago about how she was sold into child slavery and some of what happened after that.
In nearly 20 years of working as a GP, I have very rarely come across patients with chronic intractable pain, who do not have a history of trauma. It may not be necessary to talk about what has happened, but it is necessary to acknowledge that what has happened long ago can have lasting physical effects,
For patients who have suffered with chronic pain for years, discovering the links between past trauma and present suffering may very often be re-traumatising and bring on symptoms of PTSD, like nightmares and flashbacks, also worsening the pain and fatigue and other symptoms like IBS (irritable bowel syndrome). Even where we are aware of the links, there is a fear that confessing to a history of abuse will mean that fellow pain sufferers – who by this time may make up an important social/ supportive network, along with professionals who have been treating them – will reject them because their pain is somehow less ‘real’. The shame that is inherent with trauma, comes into sharp relief; shame goes with self-blame “I am to blame for the way I feel – emotionally and physically, it’s up to me to fix myself, no-one can help me now”.
Talking about the past may also be overwhelming for clinicians. Doctors exposed to stories of rape and incest, torture, domestic violence, neglect and loss, can suffer from secondary trauma. There are days when I am completely, emotionally overwhelmed. And like most GPs I don’t have a therapist of my own.
My patients and I need to be able to find hope amidst past trauma and present-day suffering, and we are discovering this together by changing our focus of attention away from ‘pathogenesis’ – the science of what makes us ill and the subject of medical education – to ‘salutogenesis’, the science of what makes us well.
At this point I would recommend you watch “What causes wellness?” an amazing talk by Harry Burns, recently chief medical officer for Scotland, in which he gives a brief history of salutogenesis grounded in the reality of trying to improve outcomes for Scotland’s most deprived citizens.
I wanted to be able to share these ideas with my patients, but 20 minutes was too long to spend watching Youtube during my consultations, so I had to find something that summed it up, that people could easily remember. The picture at the start of this piece is on the wall of my consulting room. If you hold out your left hand in front of you, fingers outstretched, looking at the palm and then look at the picture you’ll be able to imagine our conversations. Each area requires care and attention if we are to be well. Salutogenesis requires a balance; neglect one or two areas and you’ll need the others to be robust to compensate, but that’s not sustainable for long.
Beginning with the little finger, ‘Mind’ refers to feelings/ emotions/ memories, thoughts, and interpretations. Shame and anger, depression and fearfulness, heart-ache and grief, confusion, hope and despair. Taking care of your mind depends on how overwhelming (or numbed) your feelings are. For some people a good therapist is essential and the quality of the therapeutic relationship is more important than the type of therapy, but in general, the further back the problems go, the longer the therapy needs to be, and CBT probably won’t delve deep enough for long enough.
Taking care of your body definitely doesn’t require gym-membership or marathon running, many people who have experienced trauma or who suffer with pain, irritable bowels or other chronic physical symptoms have very difficult relationships with their bodies. Taking care of your body means changing those relationships, so that your body isn’t a cause of shame or dread, but something that belongs to you and does what you want it to. Yoga, dance, singing, painting, making music, arranging flowers, or baking bread can be as therapeutic as fell-running or mountain-biking. You and your body are working together, you’re enjoying what you are able to do. And you don’t need to go over painful memories.
Taking care of your biology refers to everything that you consume; food, drink, medication, supplements, alcohol and drugs, even the air that you breathe. I talk about this with patients to put medication into a holistic context – it’s one part of biology which is one finger on the hand of salutogenesis. It’s something, but it’s not, by a long way, the only thing. With a sceptical eye always open to the science of nutrition, I’m pretty confident that so far as diet is concerned, Michael Pollen is right: “Eat [real] food, not too much, mostly plants”. Most people who come to be discussing salutogenesis with me have really strained relationships with food – it’s either a punishment or a reward. Their appetite comes and goes, their weight goes up and down. They’ve been on and off diets and supplements half their lives. Helping vulnerable to stop smoking, cut down on alcohol and reduce their intake of drugs and prescribed medications can always do more to improve their wellbeing than anything new that I can prescribe.
‘Human Relationships’ is usually the most painful area. “Do you have anyone in your life who knows you well, how you love and trust, who loves and trusts you back?” is usually how I phrase the question. Loneliness is one of the worst things that anyone can suffer from. It so frequently accompanies chronic pain and chronic mental illness. Sometimes the people I ask this question say, “Apart from you?” For too many people, the GP is the ‘only normal person they know’. Helping people connect compassionately with themselves and others is almost certainly the most important thing that can be done for salutogenesis according to the Harvard Cohort Study and other research.
Human connection also requires spaces for people to meet and connect with one another. In the next video, Eric Kleinberg explains how death rates in very similar neighbourhoods varied ten-fold during a drought because some places had a lot more places where people would gather, do things together, get to know one another, and in a time of crisis, look after each other.
People for whom the dark shadow of trauma lasts into adulthood were very frequently betrayed by an adult who they trusted, who they expected to care for them. The adult may have abandoned them or abused them, and they may find it very hard to trust other people from then on out of fear of being abandoned or abused. They may blame themselves for what was done to them leading to a sense of shame. To understand shame, a sense of being profoundly un-deserving of love, kindness and respect – I have written a series of blogs – beginning here.
I really like Dr Phil Hammond’s CLANGERS – the first, and most important point is ‘Connect’ – each day I will try to like myself and reach out to others.
The thumb refers to social security, by which I mean security of housing, finance, employment, and safety from violence, intimidation and all forms of abuse. The tip of the thumb touches every other finger, with adequate social security it is so much easier to access therapy, to join a gym or go to classes, to eat healthily and to socialise. Doctors have a duty to act as social advocates and help people access the benefits they are entitled to and draw attention to the health effects of poverty. A decade of austerity and failed welfare reform means that social security has hardly been worse in living memory.
Social prescribing, derided my some GPs but greatly appreciated by others like myself, helps people to connect with other people and to access social security. With awareness of salutogenesis Social Prescribing makes a lot of sense.
Crisis management is written across the wrist because that is where so often I seen cuts that have been inflicted in a time of crisis. When the pain gets too much, self-harm and suicide are ways to bring it to an end. A crisis plan should be written, shared with others, referred to in a crisis and reviewed afterwards. It should include warning signs that a crisis is coming, people to speak to, places to go, things to do. Even if self-harm is not part of what happens in a crisis, people with chronic pain will still have days when it’s too much, when the usual strategies are insufficient. They need a crisis plan or a ‘rescue pack’ for these days. https://stayingsafe.net/ can help.
A few months ago, I faced a woman whose daughter had recently died by suicide. The woman I faced, a patient I knew well, had suffered her own terrible traumatic past and suffered with chronic pain related to connective tissue disease, trauma and grief. She wanted me to prescribe more painkillers. “What kind of pain are we treating?” I asked her, “Is it physical, emotional or grief?” She stared back at me, confrontational, “What. Is. The. Difference?” She demanded. “How can you even tell?”
I can remember the confrontation vividly. She was right. All pain affects, and is affected by physical, biological, emotional, biographical and social systems. You cannot neglect any of these areas if you want to manage pain, but when pain is overwhelming, sometimes it is easier for patients and doctors to go for a prescription, and I gave her some more Oxycodone, “We know it works”, she said, “we both know, it numbs every kind of pain.” But we also know that it’s not enough, it’s not safe and it will soon stop working. Whenever we meet we check in on all the areas on the hand together, MInd, Body, Biology, Relationships, Social Security, crisis plan. In every aspect there is room for improvement, something to be done – and in there lies hope.
“How do you cope with seeing people like me every day?” asked another patient this week. He knows what I know, that the waiting room is full of people who are full of pain and trauma. He has lived around here for 30 years. I had to think before answering and I answered carefully. “It’s true, at the end of the day I am drained. But I’ve been here long enough to have seen people through the worst of times and out the other side. Sometimes that takes weeks and sometimes it takes months or years. So I share in the suffering, but I also get to see people go through the most appalling circumstances and then recover. And that’s priceless and that’s why I’m still here and why I’m going to stay here and stick with you for as long as it takes.”
Dr Austin O’Carroll, a GP who works with homeless patients in Dublin describes this commitment and continuity to patients as ‘high fidelity’.
And in a time of professional burnout, it is important for doctors and other health professionals to think about their own salutogenesis. We are prone to burying the bits of our past that we are ashamed of, we neglect our emotional health, eat badly (especially when on call), drink too much alcohol and lose touch with our non-medical friends and family, even though we are fortunate enough to be more socially secure than most people. We are prone to over-compensate when feeling stressed, by putting all our efforts into exercise, dieting or therapy, when what we need is a balance.
I hope that the image of the hand will help me, my patients and my colleagues to focus on what we need to be well, and will give us reasons for optimism, especially for those of us working in areas of deprivation. We can always find areas where positive changes, no matter how small, are possible.
I have been a doctor for over 20 years, 5 in hospital and 15 in general practice. I have been on the receiving end of medical errors and have made complaints about my own care, and the care of family members, who are not doctors and have lacked the confidence to complain, even when complaints are clearly justified. I have also been on the receiving end of serious complaints from patients, I have been successfully sued and had cases against me investigated by the Parliamentary Health Ombudsman.
Any doctor who has practised more than a few years will know that the vast majority of medical errors are not noticed, ignored or covered up – and though the majority of these don’t cause any serious harm, a minority do. Any doctor who has practiced as long as I have, will, like me, have personally contributed to a patient’s death. Doctors are aware that most patients and their families do not complain even when they are aware that there has been an error and when they have had very reasonable grounds to complain. I have had to make complaints on my patients’ behalf because they were afraid or insufficiently literate/ articulate to do so themselves. I know that most of the time, complaints are dismissed. When patients do complain, clinicians know that the majority of complaints are not about issues involving patient harm or clinical decisions, but about problems where patients and their families feel more confident, for example; lost dentures or professional attitudes, cancelled clinics, lost results or other organisational issues. Doctors know that the worst of their colleagues seem to be immune to the complaints they deserve, while the most conscientious are prone to the most vexatious.
Dr Bawa Garba was forced, under stress to write down everything she could think of that she personally had done wrong. The person who forced her to do this wasn’t a prosecuting lawyer, but her clinical supervisor, the consultant who should have been supporting her on the day that Jack Adcock died. He did not help her think through what had happened in a place and at a time suited for reflective thinking. He made her write a list of everything that she had done wrong in a hospital canteen. He then made her upload the list as a ‘reflection’ in her educational eportfolio. This is not medical education as I or any other medical educator would practice it, but too many doctors’ experience of ‘reflection’ in medical education is shallow, critical, unsupportive and frankly, unreflective. If anyone in this case was ‘truly, exceptionally bad’ it was this doctor, Dr Stephen O’Riordan.
To make matters even worse, the media is a menace – fanning the flames of fear, pitting doctors and families against one-another and baying for vengeance and then moving on to the next story before the dust has settled.
In very little time at all doctors learn from experience that complaints are no measure of a doctor’s moral character or clinical competence. Doctors and patients learn that justice is rarely achieved.
Consequently, many doctors grow cynical, hateful of the GMC and the tabloid media and suspicious of patients. And a growing number of patients are losing trust in medical professionals.
These are problems of culture and psychology far more than they are technical and legal.
The solution must therefore involve an honest acknowledgement of the cultural milieu that doctors and patients inhabit. Doctors live in fear of patients discovering the mistakes they make and patients live in fear of being harmed. Both have good reason to think that the system is unjust. The solution must bring patients and clinicians together to have honest conversations that bring about what Richard Lehman has described as the ‘shared understanding of medicine’. It must include much greater transparency including shared medical records, patient safety reports, transparency about organisational pressures and what the NHS can afford. Patients and clinicians do need safe spaces where they can learn from mistakes apart from one another, but this should not and need not reduce the requirement to have shared learning as well. Only by making alliances with patients (contra pharma/ commercial healthcare) and by treating patients as expert partners in care (and part of the solution) rather than a burden / problem, can we change. Medical educators and supervisors must take reflection seriously and learn how to use it as a force to challenge and change medical culture for the better. Finally – as Dr JulianTudor Hart has argued, ‘Accountability must require that doctors insist that they have time to do their work properly’.
A list of books about medicine, society and more – posted here from one of my medical education wikispaces. Please send other suggestions! My intention is to keep adding to it.
Most of these books i’ve read. Many of them are old. Although I’ve linked them to Amazon for your convenience, i’d recommend you try your library (if you still have one), your local independent bookshop or second-hand from abebooks
An examination of who controls childbirth and who controls doctors
Food, politics and health:
Stuffed and Starved The best source of well researched food politics on the web. The book is highly recommended if you want to understand why a billion people are starving to death while a billion more are dying from over consumption.
For any readers based in Hackney where I work, I’m reposting this in response to Saturday’s SAFAPLACE conference at Stoke Newington Secondary School. What was an excellent conference was notable for there being no discussion about the impact of adverse childhood experiences. I’m very grateful to discover Elizabeth’s work
Throughout my twenty year career as a psychologist working in Specialist Children’s Mental Health Services (SCAMHS) two frequently repeated mantras have been amongst the biggest sources of frustration for me:
“It’s a social problem, not a mental disorder” and “the child needs to be stable to access therapy”; the latter often responded to with the helpless reply “but the child need’s therapy in order to be stable”. Indeed, much of the tension between Health and Social Care can be boiled down to these two themes.
I understand, of course, that service design and a splitting of health and social care lies at the root of this; along with a scarcity of resources and a need to carve the work up somehow. However, as a psychologist employed by health, I see a child’s context and life experiences as fundamental to their mental health and emotional wellbeing. Ironically, when it comes down to individual…
An unhappy patient comes to a doctor to offer him an illness – in the hope that this part of him, at least (the illness) may be recognizable. His proper self he believes to be unknowable. In the light of the world he is nobody: by his own lights the world is nothing”
But if the man can begin to feel recognised and such recognition may begin to include aspects of his character which he has not yet recognised himself, then the hopeless nature of his unhappiness may have been changed; he may even have the chance of being happy.
John Berger, A Fortunate Man
“One of the greatest diseases is to be nobody to anybody”
Mother Teresa
After a few weeks of watching second year medical students talk with patients I have been wondering about where, when and how empathy is lost during medical education and clinical practice.
The students enjoy talking to patients and listening to their accounts of living with diseases such as Parkinson’s disease, fibromyalgia, depression, heart disease, and diabetes. They are moved by suffering and curious about patients’ lives and their life histories. By so doing, they show natural affective and cognitive empathy.
My patients enjoy coming in – they don’t have the pressure of a 10-minute appointment within which they have to condense their symptoms into a problem to be solved for a stressed doctor who is running late. They have up to an hour of conversation without a goal in mind. They are under no pressure to impress their doctor with their weight loss or better medication compliance. Seeing the students looking more anxious and even less sure of what to say than they are themselves, they enjoy a levelling of the usual differences in power and confidence and take the opportunity to guide and reassure the students. We call them ‘patient-educators’ in recognition of their role.
Epistemic justice in healthcare is when patients have sufficient opportunity to give an account of themselves and their symptoms and the meaning and significance that they ascribe to them. We see this in the patient student encounters and encourage it.
Cognitive empathy is the ability to understand another person’s life and experiences. Affective empathy is the capacity to be emotionally moved by another person’s experiences.
With time and experience of these kinds of conversations, students learn that often patients need doctors to ask ‘the questions whose answers need to be told’. Patients won’t just volunteer information unless they can trust them. Trust can be gained by the student proving, by the questions that they ask, that they are aware that certain illnesses are associated with symptoms that might be embarrassing, experiences that may be hard to talk about, feelings that might be shameful, social stigma, prejudice and alienation. My students, my patients and I learn this together.
How, why and when is this empathy lost?
Understanding grows with experience, but opportunities for informed, compassionate, curious questioning can be squeezed out by pressures of time and the demands of specialism.
Students are expected to ‘take a structured medical history’. Conversations which once followed cues, in an attempt to understand and make sense of experiences are gradually replaced by structured interrogations guided by computer templates.
When they qualify the consultation will be less about understanding than gathering data for the health-service they are working in – because information that can be coded as data can be used for performance management, quality improvement and financial remuneration. The fruits of empathy – stories about meaning, context and experience that are unique by virtue of their subjectivity will be buried in the electronic record as ‘free-text’ – only available to those who know where to look. To satisfy the need for data, symptoms are defined as disease – headaches become migraines, dry skin – eczema, joint pains – osteoarthritis, back pain – ‘lumbar disc degeneration’, grief – depression, destitution is coded as ‘generalised anxiety’ and people who have suffered abuse are labelled with ‘personality disorders’.
In trying to visualise these different demands on a consultation, the pressure of time, the structure of a medical history, diagnostic coding, and data surveillance, I imagine a pie-chart being divided into ever smaller slices – and am reminded that over time, the patient has been squeezed out. Epistemic injustice takes over.
In time, students will become doctors who have learned to distinguish illness and diseases they can treat from those they cannot. And this, rather than the nature and degree of suffering will be their chief concern.
Affective empathy is lost when clinicians become hardened to suffering. The first patient they meet with depression or a terminal illness can be an intensely moving experience, but over time, especially if they are exhausted and hurried, and unable to attend to their own emotions or reflect with their colleagues, threatened in an unforgiving culture, they may lose their capacity to be moved.
In conclusion.
I think that empathy is lost in medical education and clinical practice. Perhaps one reason is because we don’t value the empathy our students have to begin with and don’t do enough to nurture it.
If we pay more attention to this as well as the factors that undermine it, we could do more to help it flourish.
Up until June 14th 2004 Joe was a consultant anaesthetist at a London teaching hospital. That day at work, during an operation he had a panic attack. He froze and as if in a trance, walked out of the operating theatre. The patient suffered serious harm and Joe was suspended from work and struck off the medical register. He hasn’t worked since. After he was struck off, he was referred to a psychiatrist for assessment who diagnosed Generalised Anxiety Disorder and Obsessive Compulsive Disorder and started him on the first of what was to be, over the next few years, many different psychotropic medications. He was referred for CBT (Cognitive Behavioral Therapy) and psychotherapy, which uncovered the extent of his anxiety, but did nothing to relieve his symptoms. On the day he walked out of the operating theatre, his life changed, from being outgoing and popular, he became reclusive and paranoid. His wife, a consultant surgeon continued to support the family, but they had to move to a smaller house and take their children out of private school.
I have been Joe’s GP since he left work and we meet about 3-4 times a year. Usually our meetings are quite brief. He always begins by gesturing to the waiting room and apologising for wasting my time, because there are people ‘out there’ who are much sicker than him, and I reciprocate by doing my best to assure him that I’m very glad to see him, and he is in no way wasting my time. Gradually we have established trust and a good rapport. I’ve not delved too deeply into his past before, partly because I’ve assumed that it’s something he’s been going over in therapy, and partly because our consultations are usually preoccupied with his present circumstances and working out issues with his latest drug treatment. At present he is taking two antipsychotics, two sleeping tablets, and an antidepressant. This makes me anxious and appears to have done little for his anxiety.
Unlike the transient anxiousness that naturally follows a traumatic event, when the symptoms are severe and enduring there is always a back story, but discovering it can take a very long time. The acute symptoms need to be tolerable and trust needs to be established. In writer/ editor Scott Stossell’s account of anxiety, My Age of Anxiety he asks ‘where has my anxiety come from?’ and explores, in detail, the complex aetiology which includes family history, early life experiences, human biology, social, environmental and political factors. All play a part. Psychiatrist Linda Gask asks the same question about her depression in her book, The Other Side of Silence and comes to the same conclusion. I have a strong family history of PTSD, so I have a personal interest.
I recently asked Joe where he thought his anxiety came from. “You know”, he said, referring to the panic attack in 2004. “That’s when my life changed, I was fine up until then”.
“Yes, I mean, is anxiety a family trait, were your parents, grandparents, siblings and so on anxious? Could there be an anxious gene?” Joe’s posture shifted, he folded his arms, his shoulders became more tense, his hands clenched. “No, not really, my sister perhaps, but we’re not really close”. I knew that Joe grew up in Leeds, he was the first doctor in his family and the first to go to university. I knew his sister had suffered with depression and had tried to commit suicide, but little else.
“What about your parents?”
“Not really. My dad was a bastard though. He would slap my mum about and smash the house up. My sister and I hated him”. Joe’s posture became more tense, he gritted his teeth and crossed his legs. “I remember this holiday when I was fourteen – we were going to Blackpool and I refused to go, I locked myself in my room and refused to leave. My dad tried to batter the door down, but couldn’t so he just said, ‘Fuck it, we’re going without you’. And they went without me for a week.”
Joe and I sat in silence for a while. He was curled up on the chair, trembling. Just as we imagined him as a 14 year old boy, this 50 year old anaesthetist besides me.
More came out. He has always been anxious, but was able to hide it, he threw himself into his studies and spent time his evenings in the library to avoid confronting his dad, and got into medical school where he did very well. After he qualified the anxiety became more of a problem with the pressure of work, especially when he met with emotionally distressed and traumatised patients. Anaesthetics seemed to be suited for him, but as he got older, especially, once his children began to grow up, his anxiety became harder to contain. Rather than risk being labelled he avoided going to a doctor and started using drugs from work. Soon this escalated and he was using Fentanyl (a strong opiate) until he realised he was addicted. He was trying to wean himself off and had almost succeeded, when he had the panic attack, probably due to the withdrawal effects.
“Nothing the psychiatrist has prescribed worked as well as the Fentanyl”, he said. “I was fine on that, never missed a day at work, never made a mistake. You won’t write this down, will you? I’ve never told anyone about it before.” “Didn’t they test you?” I asked. “No, and I would probably have been OK, because I was basically already doing cold turkey that day. If you could prescribe me Fentanyl now I’d stop all this other stuff, because it was the only thing that ever worked. But I know you can’t do that”.
Fentanyl like a lot of other drugs, especially opiates, psychotropics, neuroleptics and anti-depressants, for example heroin, naltrexone, Quetiapine, Pregabalin, Amitriptyline and so on, as well as alcohol – all help patients to dissociate. Dissociation is like the outer-body experience that a frightened child can achieve naturally and spontaneously as a defense. As we grow older our brains become less flexible and it becomes harder and harder to dissociate and so we use exercise, or work to cope. It is one reason why there is often a gap of decades between trauma and its aftermath. With time, it becomes harder still and strategies become addictions. For Joe, Fentanyl kept the frightened child separate from the competent anaesthetist. Nothing he has been prescribed since has been as effective.
The child that was terrified of their dad is despised for being afraid and is shameful. The high achieving child that went to university and became a successful anaesthetist is the self that is socially and personally acceptable. We all have different selves, doctor and dad, cyclist and mother and so on, but the traumatised self is despised and a source of shame and so the split is extreme and has to be maintained by any possible means of dissociation to fend off the intense anxiety that it brings.
Too much of the time I think we are content to continue to prescribe drugs to patients under the illusion that they are treating a disease rather than helping them dissociate. In some instances what we prescribe can help keep the symptoms at bay, but most of the time the anxiety persists, no matter what we prescribe.
Drugs probably do have a place in treatment, but so do top down (psychotherapeutic) and bottom up (physical) therapies that enable patients to reconnect with the traumatised self through their body and mind. We could both see how Joe’s traumatised self was inhabiting his tense and hunched body, it wasn’t just in his head. For him to recover he needs to identify the traumatised child and accept him as a part of himself. After a lifetime of shame and dissociation this is no easy task.
I’m not sure why this kind of understanding is missing from so much of medicine. Perhaps because it means shining a light on ourselves as well as our patients, and recognising that we’re not so different after all. Perhaps it’s a post-Freudian backlash and an obsession with biology and objectivity that is blind to subjectivity and experiences. Perhaps it is because financial incentives are constraining clinical curiosity – demanding that every patient narrative is recorded as a clinical code. Perhaps it is a fear of judging parents or others who are not around. Probably it is all of this and more.
One thing I am sure, is that some of the kindness and compassion that is so often missing in healthcare, in the ways we treat ourselves, our colleagues and our patients, could be recovered if we were more attentive to what makes us who we are.
It’s often assumed that it is good to talk. But talking is not without risks.
The main mental illnesses/ symptoms that patients present to me (a GP) are chronic anxiety +/- OCD and PTSD +/- chronic depression.
Chronic anxiety and chronic depression are like chronic pain, in that the symptoms persist in the absence of a causative stimulus. Which is to say that the nervous system generates and sensitizes you to anxiety/ depression/ pain of its own accord. It is not to say that if you have chronic pain, it won’t help to have me stop stepping on your toes, or if you have chronic depression it won’t help to have financial security or if you have chronic anxiety it won’t help to get away from a violent partner.
Without a clear explanation for these chronic symptoms, sufferers and clinicians inevitably spend a lot of time alone and together trying to figure them out. Uncertainty abounds.
Care of patients with chronic symptoms requires time to build trust and a therapeutic relationship. This develops through talking (dialogue). What we discover by talking is what it’s like (the phenomenology), where it comes from (the biology and the biography) and what it means (the hermeneutics).
Trust and time
Feminist, activist and professor of psychiatry Judith Herman warns that we may push for more facts before the patient has had time to deal with the emotional impact of the facts already known. Before exploring the past, it’s important to understand the present. Cognitive empathy is informed curiosity – asking questions that prove we’ve got an idea of just how bad anxiety and depression can be, but are sincere in wanting to know what it’s like specifically for the person in front of us. As one of my patients told my students, “I’m not going to open up if you don’t know where to look”
Quite frequently the physical symptoms of anxiety are so severe that it’s barely possible to get into the psychological side of things. Incontinence, breathlessness, chest pain, severe headaches, spasms and so on need to be attended to first. This can take time.
Once these are within reasonable limits the patient (and the doctor) need to be able to bear the emotions. Joanne Bourke, historian of Pain, says that the problem with pain [suffering] isn’t just that it’s hard to talk about it, but that it’s painful for the listener. I think I can bear to bear witness to suffering, but it is exhausting emotional labour. We have limits on how much we can hear, but as professionals we need to work on these.
Next, the patient needs to have authority over her memories; she needs to be able to choose what to remember and what to put aside. It’s not up to the doctor to decide.
There may not be a story to tell
Traumatic experiences happen when stress hormones like adrenaline and cortisol are surging. Because of adrenaline the experiences are only partially stored as memories and because of cortisol the storage is disorganised.
Experiences become stories by the acts of telling and re-telling. Traumatic events are not the stuff of anecdotes, they aren’t turned into stories, mostly they are the symptoms of fear, agitation, arousal, dread, pain, bloating, fatigue, sweating and palpitations – The Body Keeps the Score. Recalling traumatic experiences is traumatic – which is why the preconditions above matter. The consequence of all this is that there may not be ‘a story’ to tell, let alone one that makes sense. At least not to begin with.
Telling someone that you are suicidal, that you have everything in place to take your life – is a risky strategy – good ways to respond, from the perspective of someone who knows what it’s like are in this brilliant blog which I’ve had reason to refer to already, twice this week. But an unsympathetic ear, or a panicked response – can be catastrophic.
Working back from present symptoms to past experiences takes time. This week I spoke to two patients I have known for about 10 years and started hearing about their trauma for the first time. Without continuity of care, and trust that can develop over time, these kinds of conversations might never happen.
Every patient has their own unique story
Underlying their anxiety and depression, one person will have a strong genetic prediposition with a secure childhood, another will have have suffered abuse and another will have suffered significant losses in early life, for other the cause will remain a mystery. The aetiology of mental suffering is complex and varied. How much genes, attachment, experiences and so on contribute to each person’s presenting symptoms can be hard to judge. I think it’s important to help patients figure out what’s significant to them, bearing in mind that self-blame can be predominant and we can help to shift that. Often though, there is someone to blame; too many children are abused and too few of those responsible are bought to justice. But we have to avoid blaming others when there wasn’t abuse and when it’s not clear what has happened.
Groups are often very powerful – validating, empathic, non-judgemental – far more so than professionals. It is tempting for professionals to try to ‘fix’ people’s problems when what they need is to be cared for, because a lifetime of anxiety and depression cannot be cured. Talking may be much easier with people who share their experiences, but without respect and facilitation groups can be undermining.
Responsiblity
Being mentally ill can make people very vulnerable to exploitation, fearful and acutely sensitive to the ways that other people respond to what they have to say. These feelings are not just symptoms of their illness, but an entirely rational response to the ways they have been treated in the past. Talking is good, but more of the responsibility needs to lie with the listener.
Talking is not enough
Once you’ve talked to more than a few people suffering from mental illnesses, it’s obvious that social injustice, violence and stigma, not only cause illnesses, but worsen them and impede recovery. Political action is imperative. This is why so many people who work in this field, like Judith Herman, Jay Watts and many more are clinicians and activists. If you’re good enough to listen, you need to take action as well.
We need properly funded mental health services, and well-trained health professionals. We need Trauma-informed health services throughout the NHS. Talking does help, but we need more treatment too.
One of the most haunting images from my time as a junior doctor working in Hackney in the mid-1990s was in an A&E (emergency) department while we tried to resuscitate a man in his 40s. In the corner of the room stood two young children – probably about the same age mine are now, 6-8 years old. They stood and stared in silence, watching us trying to save their dad. He was covered in blood and bile, his body yellow with jaundice, veins visible on his abdomen and torso from advanced, alcoholic liver disease. His wife was in another part of the department, so intoxicated she couldn’t stand, barely conscious and unaware of what was happening to her husband and children. The children were eerily impassive. The ambulance crew told us that when they arrived at their flat, they were trying to wake their dad while their mum lay unconscious, snoring in the next room. The flat was squalid and the children were obviously severely neglected. By now they will be in their mid to late 20s, assuming they are still alive, possibly with kids of their own. I wonder what became of them.
A lot of my time in A&E in south east London was spent with young people, mostly women and girls who cut themselves or took overdoses. I absorbed the culture of my workplace – where they were usually treated as ‘timewasters’ and where ‘PD’ which stands for ‘Personality Disorder’ was a term of abuse. I quickly became aware that all of them had been abused (usually sexually) or neglected severely, but I struggled to find anyone who knew what we could do to help, and faced with our own helplessness we continued to patch them up, push them away, and complain about them wasting our time. I remember one night meeting a teenage girl who wanted treatment for sexually transmitted infections, she refused to be examined, protesting that it was too sore, too smelly and too embarrassing. She looked terrified. I was the only doctor in a busy department in the middle of the night – she slipped away before I had an opportunity to find out any more.
I rotated between junior doctor posts, driven by a mixture of curiosity and an inability to commit to a specialty at an early age. After A&E I worked as a junior surgeon and gynaecologist where I met dozens of patients (also mostly young women) whose enormous hospital records documented their repeated admissions, investigations and surgical procedures. We couldn’t explain their abdominal pain and bloating, pelvic pain and unexplained severe constipation or incontinence. Some of them also cut themselves, but mostly we examined the scars that criss-crossed their abdomens made by surgeons, looking for the source of their symptoms in the organs underneath.
I spent just 3 months working part-time in sexual health, barely long-enough to wonder why just a few young people (again, mostly women) accounted for such a high proportion of the visits.
As a young, naive paediatrician I saw kids with ADHD and other conduct disorders, many of whom had a dysfunctional home environment. Some were adopted, but we were strangely uncurious about what had happened to them before they were adopted. I met countless parents who were overwhelmingly anxious, who bought their children to hospital week in, week out. Some seemed to spend every Friday night in A&E. I focussed on the children and it hardly ever crossed my mind to think about what had happened in their own lives, or might still be happening, that rendered them so fearful.
I spent 6 months as a junior psychiatrist where I had a little more time to listen to patients, but many refused to talk for long to a doctor they had never met before and might never meet again. I struggled to find ways to find the information that mattered most to the patients I read their extensive discharge summaries but struggled to find out which events were the most significant in their lives. It was clear that mental ill health had a complex aetiology – which is to say that similar illness were clustered in families, were affected by experiences, and were worsened by deprivation, intoxication and isolation, most of which we had no ability to influence. For some people psychosis struck someone in the most stable of social circumstances, but for most it was chaos superimposed on chaos. We prescribed every new drug that came on the market, usually on the basis of the earliest trials and negligible evidence of benefit. The side effects – “They’ll make you fat and impotent!” one patient yelled across the ward as I tried to persuade another to try them, were more predictable than the benefits.
As time went on I realised that if I wanted to understand why people suffered from unexplained symptoms, chronic pain, anxiety, depression and psychosis I would need work somewhere where continuity of care was valued and protected.
For most of the last 17 years, I’ve been a GP working in Hackney in East London. We serve an increasingly economically diverse, but still very deprived, young, socio-culturally mixed group of patients.
A lot of what many people would consider to be ‘normal general practice’ – managing diabetes, hypertension, heart disease, minor illnesses and so on, is managed by practice nurses, specialist nurses, clinical pharmacists, GP trainees and salaried doctors. GPs like myself who have been around for long enough to develop therapeutic relationships with patients spend most of our time with patients who suffer from chronic pain, medically unexplained symptoms, addiction, eating disorders, severe obesity, self-harm, suicidal thoughts and mental health disorders; especially chronic anxiety, chronic depression, OCD, bipolar and personality disorders. Among them are our patients with the worst diabetic complications, the most symptomatic heart-failure, the most brittle asthma and out of control hypertension. They are the same patients who I met again and again as a junior doctor, who bewildered and frustrated me and my colleagues. They are still the patients who attend A&E most frequently and are most likely to fail to attend routine reviews. If they are not asking me to give them something for their chronic pain, debilitating anxiety and insomnia, for weight loss or breathlessness they need me to write reports for housing or benefits assessments. I, and thousands of doctors like me, spend every day caring for patients like this. One thing I have only very recently learned, is that Trauma is embodied.
What is extraordinary, and to be frank, a betrayal of patients and clinicians on the part of those responsible for medical education is that we never talked about, much less seriously taught about the lasting effects of trauma. We were taught that diseases were due to the interaction of human biology and the environment, but human experiences were barely part of the picture.
Julian Tudor Hart worked for over 40 years in the same practice in the Welsh Valleys and saw the same community after the mining industry closed down. Not only did unhealthy lifestyles and mental illnesses proliferate, but so did domestic violence and incest. Without meaning and purpose, for some people, morality collapsed.
For John Launer, GP educator and narrative medicine pioneer, medically unexplained symptoms are better understood as ‘medically unexplored stories’. Most GPs, especially those who work in deprived areas, bare witness every day to their patients’ accounts of trauma; including physical abuse and neglect; parents who were, because of alcoholism, drug abuse or mental illness unable to care for their own children in their earliest years; stories of material and emotional deprivation, abandonment and loss, domestic violence, crime and imprisonment and with shocking frequency, child abuse. Trauma begets trauma so that people rendered vulnerable by trauma in childhood are very frequently victims of violence and abuse in later life. Survivors of trauma use drugs and alcohol to cope with the aftermath, then find themselves involved with crime which leads to imprisonment and homelessness and further cycles of alienation and despair.
People whose work does not involved repeated encounters with survivors of trauma frequently either cannot believe, or refuse to believe how common it is. For years it’s been assumed that people invented stories of trauma to excuse bad behaviour. The medical profession bears a lot of responsibility for this, largely ignoring the psychological consequences of rape until the last 30 years.
In 1896, Freud presented the detailed case histories of 18 women with ‘hysteria’ – what might these days be labelled ‘Emotionally Unstable Personality disorder’. In every case the women described childhood sexual abuse. Freud thought that he had found the ‘Caput Nili’, the source, of hysteria, and presented his findings in anticipation of fame and possibly fortune. What he failed to anticipate was that the upper echelons of Viennese society were not prepared to accept that women with hysteria could be telling the truth and in so doing, implicating their own, privileged social circles. Freud was sent away to come up with another, more acceptable theory. His insights were buried and forgotten for most of the 20th century.
Ruby is imposing. She is six-foot-tall and one hundred and thirty kilogrammes. She rarely goes out, but when she does she dresses up – lots of gold jewellery – pink Doctor Martin boots, a huge, bright, African print dress and a gold, sequined stick. “Do you know how long it took me to get to know and trust my last doctor?” she has asked me, rhetorically, several times since we first met, about 10 years ago, after her last GP of 20 years left. “You know what I’m looking for in a doctor?” she asked, “Someone who looks comfortable when I’m sat in front of them”. How many times, I wondered, have patients looked to a doctor for help and empathy and seen fearfulness, frustration, confusion or worse; moral indignation or disgust. I know it happens. Dozens of studies have shown that the attitudes of professionals towards patients who are overweight, who self-harm, and who have personality disorders are at least as prejudiced as the non-medical public. I know I’ve done it before. But I think I’m more aware of it now, and I’m much better prepared to bear witness to trauma.
Ruby was sexually abused by her grandfather from the age of 6 to 9. When she told her mother, she didn’t believe her, her grandfather continued to visit and the abuse went on. When he stopped abusing Ruby, he started abusing her younger sister. Ruby started eating to protect herself – to smother her emotions, to make herself less attractive, to make herself more imposing and better able to defend herself. She fought at school all the time and was repeatedly excluded. She was never asked about abuse, but if she was, she would almost certainly have denied it. Happy kids don’t suddenly double in size and start fighting unless something terrible has happened. So many adults I look after who can recall the day when they suddenly stopped being a ‘normal child’.
In 1987, Vincent Felitti a doctor running a weight loss programme for severely obese adults in the US mistakenly asked a woman how much she weighed, instead of how old she was, when she had her first sexual experience. “Forty pounds”, she replied. “With my father”. He went on to interview nearly 300 other women attending the clinic and discovered that most of them had been sexually abused. He presented the findings to the American Obesity Association in 1990 and the response was almost the same as Freud had nearly 100 years before:
When he finished, one of the experts stood up and blasted him. “He told me I was naïve to believe my patients, that it was commonly understood by those more familiar with such matters that these patient statements were fabrications to provide a cover explanation for failed lives!”
We don’t like to talk about trauma because it’s very hard to accept that something so horrific should be so common, and the perpetrators, who are usually known, so normal. Most perpetrators of sexual violence, child abuse, domestic violence and rape, have no history of trauma of their own, and no evidence of mental illness. Coming to terms with this very uncomfortable fact means accepting that there is something very, very wrong with the way we are raising young men.
The doctors running the obesity clinic developed their line of questioning to include 10 categories of Adverse Childhood experiences listed below.
Not all categories are equally traumatising; the severity and duration of adverse experience is important in determining the extent of traumatic aftermath – the ‘trauma world’. 30-36% of people have no ACEs, but different-types of adversity go together, for example alcoholism, physical abuse and violent behaviour. The higher your ACE score the greater your risk of physical and mental ill-health and social disadvantage in the future. An ACE score of 4 or more increases the risk of heart disease 3-fold and Type 2 diabetes 4-fold. People with an ACE score of 4 or more are 6 times more likely to smoke and 14 times more likely to have experienced violence in the last 12 months. People with an ACE score of 6 or more have a life expectancy of 20 years less than those with a score of 0 because of illness, violence and suicide.
Diagnostic difficulties
Clinicians should suspect trauma in people whose symptoms and behaviour are like those I’ve described, but we need to be careful not to blame every symptom on trauma. The symptoms and behaviours associated with trauma can occur in people who have not suffered trauma. The embodiment of trauma causes lasting physical changes to the brain and body, which combined with self-destructive habits, hugely increases the risk of serious diseases. We must not forget about biology while we attend to biography. Multiple physical symptoms and associated hyper-vigilance can make it very hard for survivors and clinicians to recognise when symptoms are not a manifestation of trauma. Knowing which symptoms to investigate, and how far to go needs an experienced clinician, but often, because survivors are seen as ‘difficult’ they end up with the least experienced.
Disconnection, Fearfulness and shame: The Trauma World
While the ACE studies show that trauma is associated with a wide spectrum of illness and adversity in later life, they fall short of explaining how or why this happens. The aftermath of trauma, for those who lack the good fortune to be sufficiently resilient, is a world of disconnection, fearfulness and shame, the ‘Trauma world’.
Disconnection / dissociation.
Many people who have survived childhood abuse describe how they could separate themselves, from the act by ‘an outer body experience’ –
“He’s inside me and it hurts. It’s a huge shock on every level. And I know that it’s not right. Can’t be right. So I leave my body, floating out of it and up to the ceiling where I watch myself until it becomes too much even from there, an then I fly out of the room, straight though the closed doors and off to safety. It was an inexplicably brilliant feeling. What kid doesn’t want to be able to fly? And it felt utterly real. I was, to all intents and purposes, quite literally flying. Weightless, detached, free. It happened every time and I didn’t ever question it. I just felt grateful for the reprieve, the experience, the free high”. James Rhodes, Instrumental.
Whilst children are quite adept at this and with practice can slip into states of disconnection quite quickly, it is harder for adults. The aftermath of trauma, the trauma world, often persists or may even manifest for the first time, years after the abuse has ended. Alcohol is one of the most potent and effective dissociating drugs. Addiction specialist Hanna Pickard describes, in a radio 4 interview, the occasion when she found herself in the back of an ambulance with a broken shoulder having been knocked off her bicycle in a crash that also involved her two young children. The effect of the morphine was to profoundly dissociate her from the pain in her shoulder. She understood then how if she had also been suffering the unbearable agony of her children dying in the accident, it would dissociated her from that pain as well. Sedative drugs prescribed to treat chronic pain and chronic anxiety – opiates, anti-epileptics, antidepressants and benzopdiazepines are almost entirely unselective – they even numb the pain of trauma, hopelessness and despair.
We can disconnect from memories and aspects of ourselves that we cannot bear or are afraid to acknowledge without drugs or alcohol. For some people, excessive work or exercise can achieve similar effects, especially when it involves pain and self-sacrifice and can even drive exceptional success in academic or athletic performance. But in spite of this, because trauma profoundly affects the sense of being worthy of love, attention and respect, this success is rarely matched by positive relationships with other people.
One of the ways that people who have experienced trauma, especially abuse, rationalise what has happened is by blaming themselves.
The overwhelming sense of being deeply flawed and unworthy of care and attention makes it very hard to convince people who have suffered trauma that they deserve the care that they are entitled to. They can be very hard to engage with care, and are often excluded because they can be chaotic and have different priorities – safety, money, housing and so on, to clinicians. Self-harm through neglect, and unhealthy behaviours are much more prevalent among people who have experienced trauma, as is more direct self-harm like cutting and suicide.
Fearfulness
Doctors, nurses, receptionists and others who work with people who have experienced trauma and suffer the trauma world that comprises trauma’s aftermath, know very well how overwhelming and contagious patients who suffer severe anxiety can be. From repeat attendances, especially to A&E and out of hours, to panic attacks and aggressive behaviour, the emotional labour, sometimes referred to as secondary trauma, of caring for people who are very chronically, severely fearful is exhausting. A child who has experienced trauma is constantly vigilant, always on edge, prepared for fight or flight at all times. This constant tension and hypervigilance leads to high-levels of hormones like cortisol, adrenaline and noradrenaline, tense physical posturing or the opposite – cowering; hypertension, breathlessness, chest tightness, irritable bowels; and over time chronic pain, heart-disease and eating disorders – especially when they represent a battle for self-control. The constant fearfulness becomes an inseparable part of the traumatised person’s identity, so that it becomes impossible to relate the physical symptoms to ‘anxiety about a thing’. Somatic symptoms lead to the fear that a fear that there is something wrong, some awful disease in their stomach, chest, brain, or wherever the symptoms are felt. Faced with patients whose anxiety and physical symptoms are overwhelming, clinicians frequently resort to medical investigations, often in a futile attempt at reassurance, to allay their own anxiety or because it’s easier to talk about the diseases they don’t have than the stories they do. Because the risk of biological disease is so much higher for these patients, the tests aren’t entirely without justification, but most of the time they serve to distract rather than reveal the underlying causes.
Feelings of safety, security and trust in other people are laid down in the very earliest years of life. Deprived of this, anxious babies become frightened children and fearful adults. Desperate for human connection, they often make intense attachments with others, and then terrified that they will be broken off, in part because of their own intensity, they sabotage the relationship before the other person lets them down – as has happened so many times before.
Resilience and protective factors
Because resilience is conflated with moral character- to be resilient is to be seen to be courageous, stoical and strong – the flip-side is that people who suffer more are assumed to be less resilient. All survivors of trauma have have survived by virtue of extraordinary resilience. Those who suffer more, don’t lack resilience,and certainly don’t lack moral character, but suffer more because their trauma was more severe, more prolonged or incurred at a younger age or more vulnerable time in their lives.
Another reason for suffering more is a lack of protective social factors. Almost certainly, but very difficult to prove, the most important is a long-term relationship with an emotionally stable adult. The worse the abuse, and the younger it starts, the harder it is for people to achieve this – an inability to trust other people becomes part of their personality. Afraid that their victims might develop a relationship with anyone else, abusers frequently do whatever they can to stop this happening. Many GPs find ourselves in the position of being the ‘only emotionally stable adult in a victim’s life’. I went for years knowing, or at least suspecting that this was the case before understanding the links with trauma.
Socioeconomic factors can be protective – but only up to a point, as the many survivors of trauma from privileged backgrounds have testified. But severe deprivation can be traumatic in and of itself and exacerbate the effects of other types of trauma.
Trauma in contexts of deprivation may lead to survivors spending their lives being shunted from one crisis service to another, from temporary accommodation to emergency shelter, from one GP to the next. Just as they’ve begun to trust and confide in someone, they are uprooted and moved on. To make matters worse, doctors are taught to be afraid of dependency, to view it as ‘disempowering’ patients, and/ or as a symptom of their own unhealthy/unprofessional need for human connection. Some neglect continuity of care, others actively avoid it. For Arthur Frank, medical sociologist and anthropologist, ‘The structured disruption of continuity of relational care is more than an organisation problem; it is a moral failure of health care, deforming who patients and clinicians can be to and for each other’. In an age where independence and individual autonomy are moral virtues, it is shameful to admit that you need human connection.
Being able to make sense of what happened is often very hard. Abuse is so often done by people who should have provided kindness and protection to a vulnerable young person. It is heartbreaking, but understandable that victims frequently rationalise this by thinking, ‘it must have been something about me, something I did, or said – it must have been, at least in part, if not wholly, my fault’. Abusers sense this and feed into it, telling their victims that they are getting what they deserve until eventually they believe it. Finding different ways of making sense of abuse – perhaps years after it has happened, can be extraordinarily difficult and can require long-term therapy. For some people though, I believe that what happens, over repeated short appointments with a GP, perhaps over many years, is that new narratives are co-created, making sense of what happened in different ways.
Trauma is disempowering; a sense of self control is wrenched, often violently away. Fearfulness and disconnection add to the identity of a body out of control. In abusive relationships the victim is rendered powerless. If the victim is helped to gain a sense of (and of course, actual) control, it helps enormously.
Recovery
Like all healthcare professionals, and especially those who work in deprived areas I care for the survivors of trauma every day. It helps to know as much as possible what evidence there is for recovery.
The slide above is adapted from Judith Herman and Bessel Van der Kolk. It can take years to develop enough trust with a patient to talk about trauma, during which time millions of pounds might be spent investigating and treating their physical symptoms and mental health. The costs to the NHS and other healthcare systems worldwide have never, to my knowledge been investigated. Without the opportunity to develop trusting, long-term, therapeutic relationships, many patients are denied the opportunity of recovery. Van der Kolk warns strongly against assuming that there is ‘a’ treatment for trauma, there are too many different types affecting too many people in too many different ways for one to be sufficient. Because trauma affects both body and mind, treatments that attend to both are very often required. It must also be remembered that trauma is just one of a number of contributory factors to many diseases, and we must not overlook the others, or assume that trauma alone is responsible. Autistic spectrum disorders can be mistaken for trauma because of problems with social interaction, anxiety, sensitivity to sound/ light/ touch and impaired motor coordination are common features of both.
The quality of therapeutic relationship is more important than the type of therapy, but it is almost impossible for the rational self to talk the emotional/ physical self out of its own reality, which is why CBT often fails.
Prevention
Vulnerability to trauma begins before birth and is especially important during the first 2 years of life. Childhood poverty in the UK has been rising for years and is among the worst in the developed world. Programmes to ensure children get the best possible start in life- like Sure Start have been cut or scrapped. Health visitors are completely overwhelmed as are drug and alcohol services. It seems that there will probably be even more victims of trauma in the future. We need to raise awareness among professionals, the public and policy makers. We need advocacy and activism from professionals. We need a social safety net that is not so inadequate that people are forced into destitution or in which a life of intoxication is preferable to the impoverished, hopeless alternative.
Trauma informed care
Care for people who have experienced trauma needs to be based on evidence and compassion and combined with advocacy and activism
The role of the GP
GPs are not trained therapists, but the work that we do is very often therapeutic. A compassionate curiosity informed by knowledge of the ‘trauma world’ enables empathy, which is described by Leslie Jamison, author of ‘The Empathy Exams’ as, ‘asking the questions whose answers need to be told’.
Treatment begins with the sense of being listened to by someone whose intention is to understand. If the therapist (GP) can take in something of the magnitude of what has happened to the patient, internally and externally, without being totally overwhelmed by it, there is a hope once more of re-establishing a world with meaning in it.
Caroline Garland (2005)
The importance of a containment of this kind cannot be overestimated. In consultations, a therapist is required to take in overwhelming experiences without becoming overwhelmed him/ herself. Profound anxieties and hostility are part of what the trauma patient is unable to hear. The therapist needs to register and contain such feelings sufficiently if the patient is going to come to contain and integrate such feelings him /herself.
This demonstrates that the therapeutic relationship, rather than the event itself is central for the consultation. Joanne Stubley Trauma (2012)
Finally
Learning about trauma has completely transformed my practice, helping me to make sense of so much that has frustrated, worried and exhausted me for years. I am now committed to sharing the lessons with other healthcare professionals, beginning with my whole practice team – from the receptionists who frequently face hostility and unpredictable behaviour, to the secretaries who type reports full of traumatic detail, the nurses who see them for intimate examinations and the doctors who struggle with their inexplicable symptoms. Struggling with patients who have suffered trauma can inflict trauma on those whose job it is to care – both because of the intensity of experiences and because their own trauma may be triggered.
My hope is that the NHS can act with science and compassion combined with advocacy and activism to lessen the amount of trauma being inflicted and improved the care of those who have survived.
Podcast – a 40 minute interview I gave about this subject with some new thoughts, in March 2018 https://soundcloud.com/jane-mulcahy/dr-jonathan-tomlinson-law-and-justice-interview
Social determinants of health, multi-morbidity, cradle to grave care, and Sylvia who is 90 years old and spent the last decade caring for her husband with dementia and now wants me to help her join him in heaven.
Child health, mental health, sexual health, trans health and Mehmet who is only 21 years old and will not use insulin for his type 1 diabetes and is blind and dying from renal failure.
Home care and advocacy for twins, Sam and Fred who have learning difficulties, are destitute and are trying to survive.
Ever-changing targets, financial pressures, press hostility and a wonderful team and the chance to innovate.
Knowing patients for years and growing to love and respect those with whom we’ve struggled most of all.
A deep well of local knowledge and a parsimonious custodian of healthcare resources.
A growing realisation that ‘doctor’ is an inadequate description of a GP.
150 words.
This is my contribution to #GP150w – a wonderful initiative by Dr Jamie Hynes
A new service has been set up in our local hospital and they have asked if they can visit our GP practice to tell us about it and they are offering us some ‘teaching’ – presumably related to their specialty.
We are going to invite them, but rather than replicate the usual format for these meetings we (I) thought we might tell them what, from our perspective, an ideal specialist service might provide.
This is a generic wish list, for any specialty. Hopefully patients, GPs, specialists, commissioners and other healthcare professionals might offer their own suggestions.
Firstly we want a website, accessible to patients and professionals for your service with all the relevant information, which should include the following:
Contact details: Travel, phone numbers for appointments, cancellations, and other queries. An email address or contact form
Links to patient-information including self-care, self-referral options, local support, help-lines, patient-forums, etc.
Links to information for carers and advocates
Up to date guidelines, and shared-decision making tools for patients and professionals
Quantitative data: how many patients are you seeing, how long are they waiting for an appointment? How long do they wait when they get there?
Your commitment to patient-centred care: How are the material, organizational and interactional aspects of your service, ‘patient centred?’
Patient and clinician feedback: It should be possible for patients and professionals to leave feedback via your website. You should analyse it and provide a monthly report including your proposed action
Quality measures. These should include:
Patient-reported outcomes and long-term follow up – we want to know how long your interventions are effective for
Safety reports: a monthly or even quarterly summary would do
Patient satisfaction surveys: Quarterly or biannually?
Staff satisfaction surveys: Once or twice a year? We want to know that we’re referring to a service that cares about its staff
I’ve tried to keep this list short. No service I know comes anywhere close to this. Patients have to trust that we will refer them to services that will take good care of them but trust is not enough.
Thanks to Phil Cavel who has blogged his experience of spinal surgery for prompting me to write this. If you’re looking for a new, very special bicycle, he’s your man.
London Health Emergency
Founded in the autumn of 1983, London Health Emergency is the country’s biggest and longest-running pressure group in defence of the NHS.


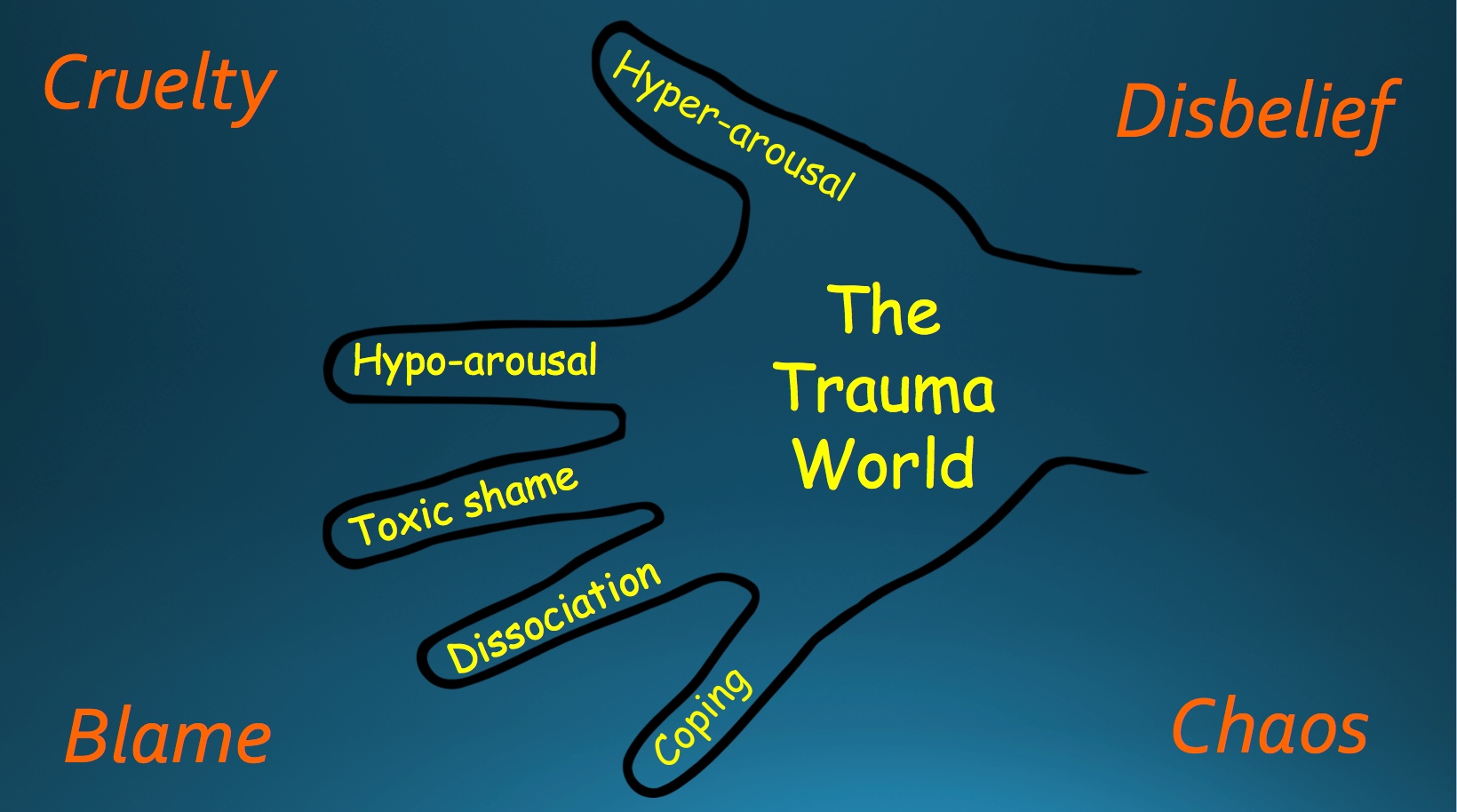

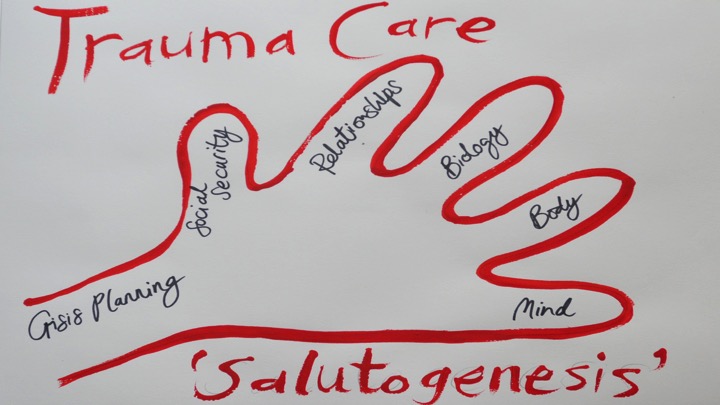
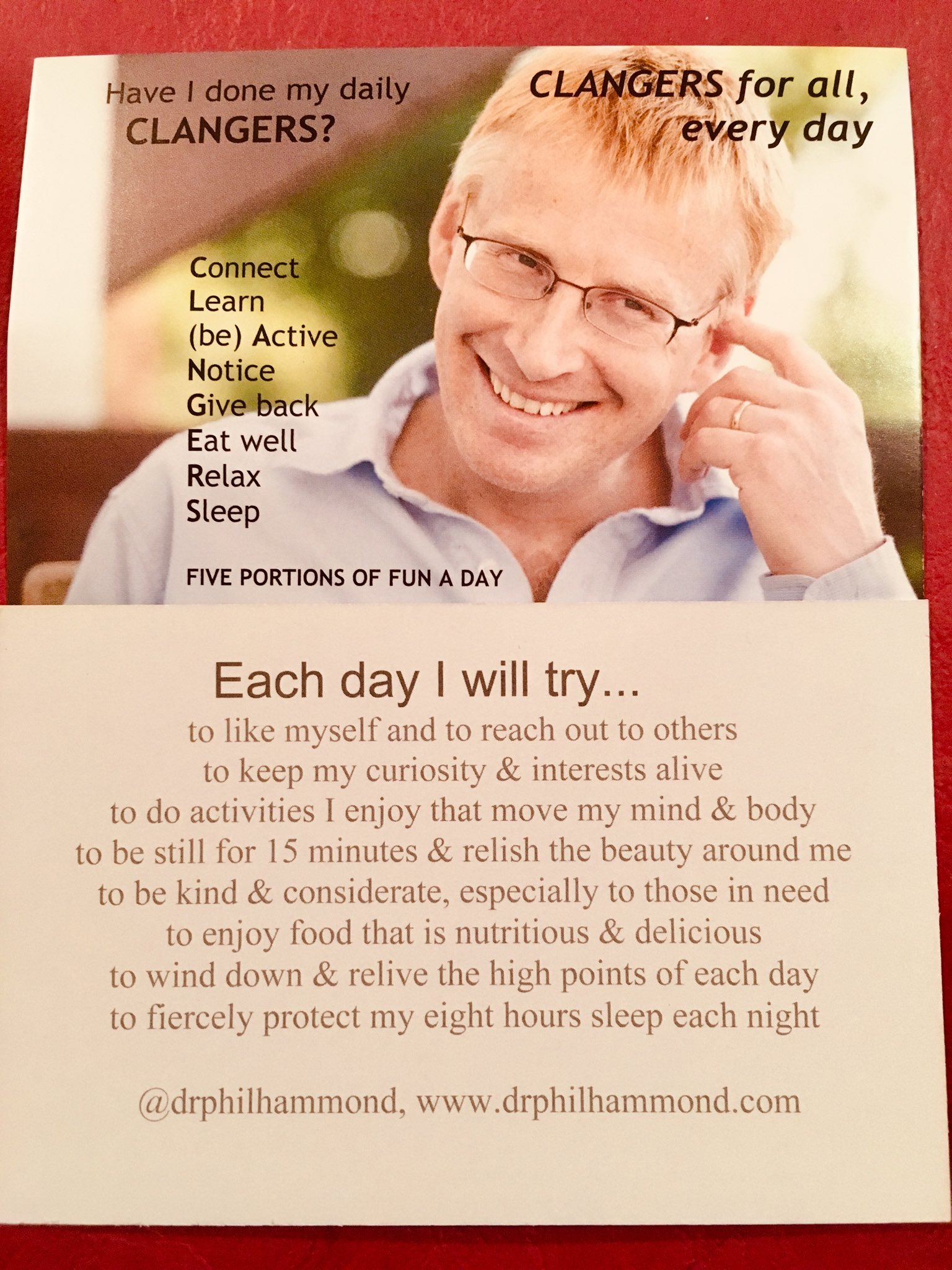
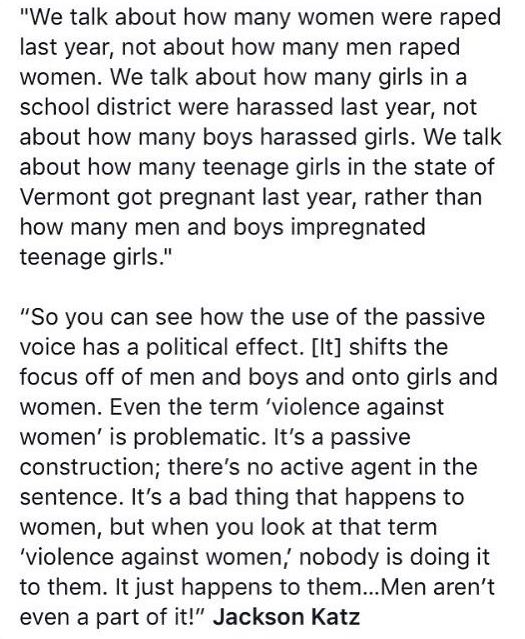
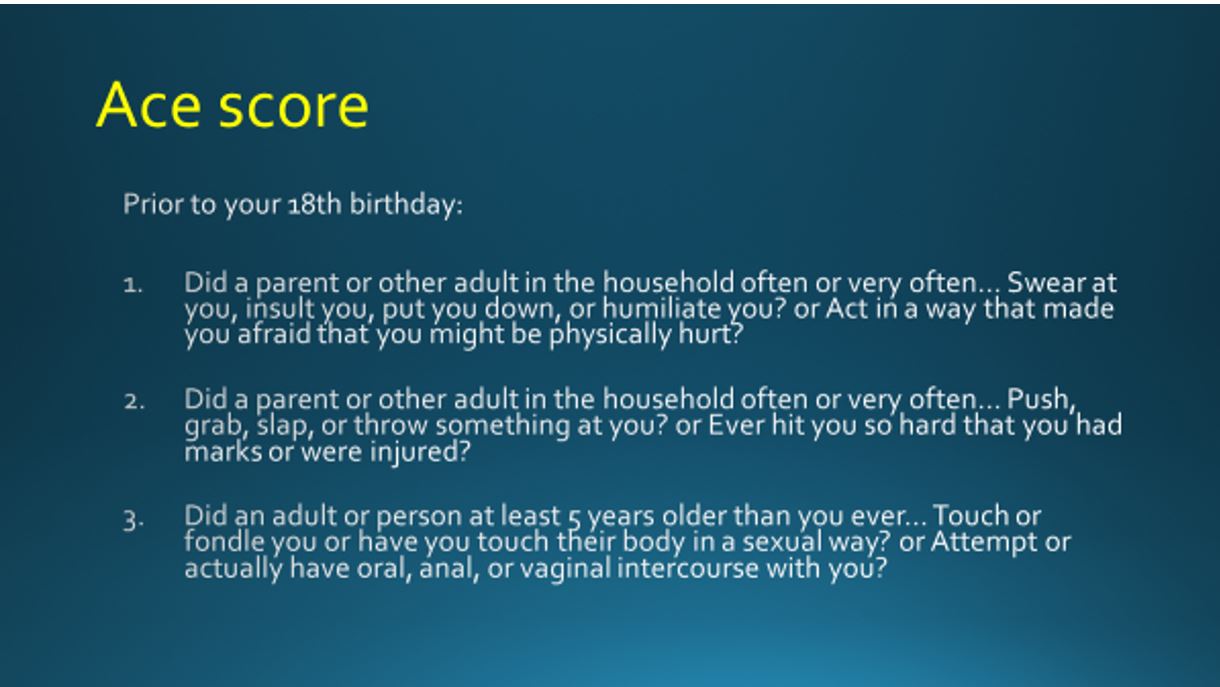
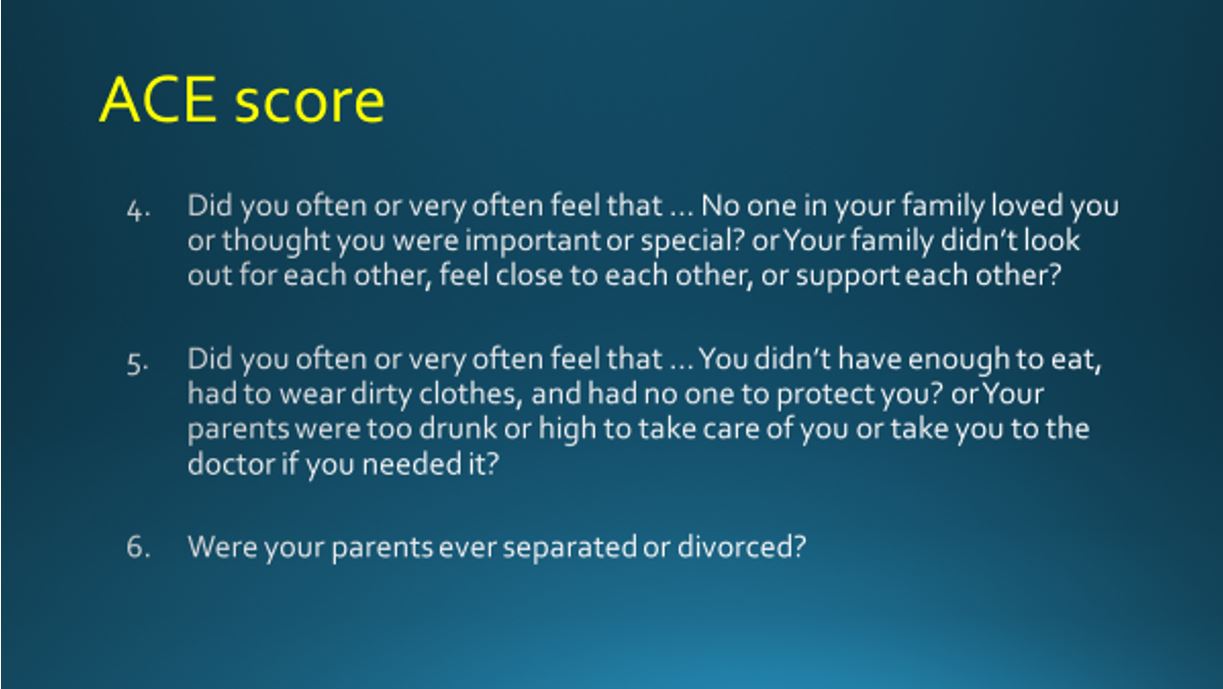
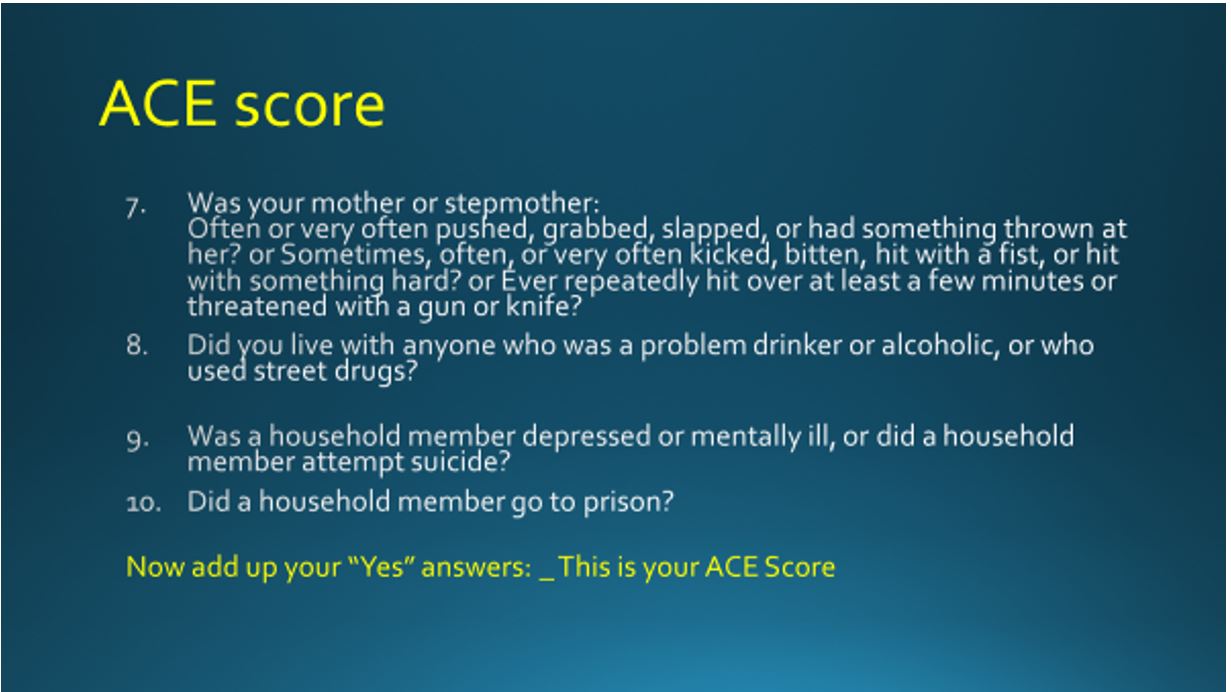
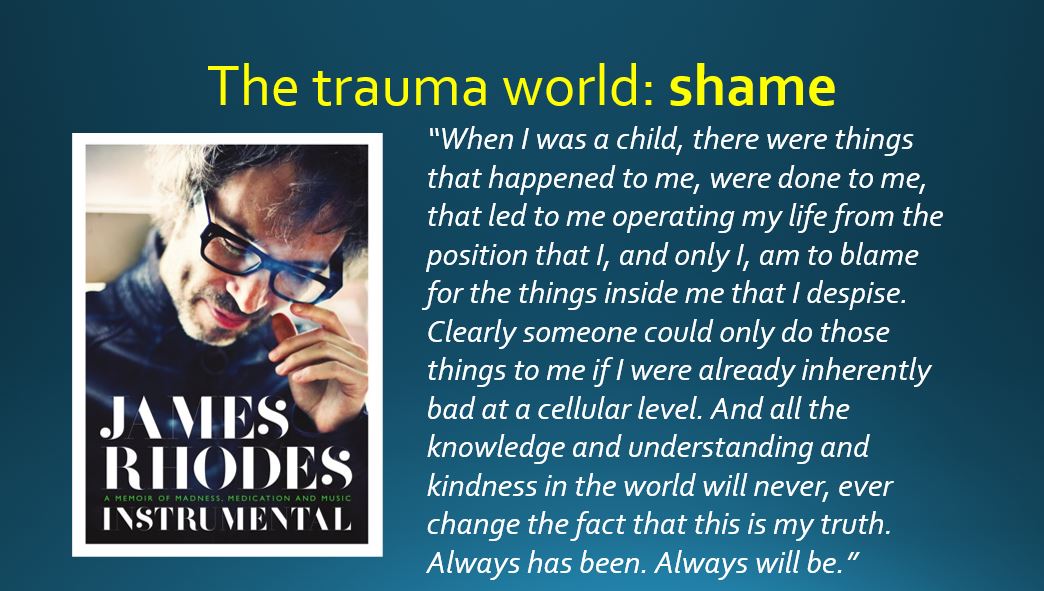
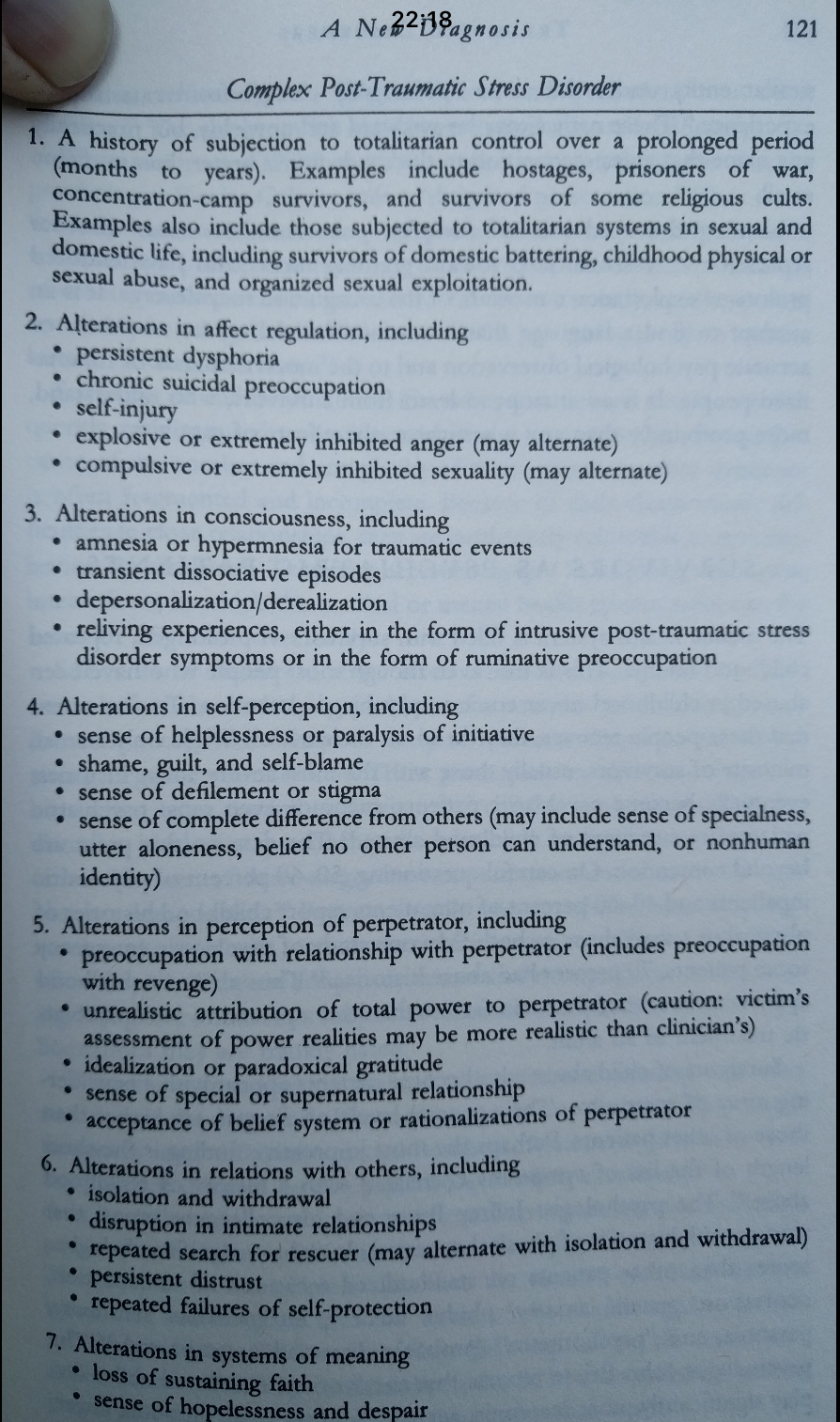

General:
Henry E. Sigerist: Medical Historian and Social Visionary
Medicine and society:
Medicine and science in the media:
The media:
Hoxton history:
General practice:
Doctors and patients:
Medicine and politics:
Markets
Pregnancy and childbirth:
An examination of who controls childbirth and who controls doctors
Food, politics and health:
Health promotion
Poverty and medicine:
Pain: history and culture:
Pharma
Medicalisation
Dying
Mental health:
Medical ethics
Medicine and History
Misc